Department of Immunology, Universidad Autonoma de Nuevo Leon, UANL, School of Medicine and University Hospital, Monterrey Nuevo Leon, Mexico.
BMC Infect Dis. 2012 Jan 20;12:15. doi: 10.1186/1471-2334-12-15.
Community-acquired pneumonia (CAP) is considered the most important cause of death from infectious disease in developed countries. Severity assessment scores partially address the difficulties in identifying high-risk patients. A lack of specific and valid pathophysiologic severity markers affect early and effective sepsis therapy. HMGB-1, sRAGE and RAGE have been involved in sepsis and their potential as severity markers has been proposed. The aim of this study was to evaluate HMGB-1, RAGE and sRAGE levels in patients with CAP-associated sepsis and determine their possible association with clinical outcome.
We evaluated 33 patients with CAP-associated sepsis admitted to the emergency room and followed in the medical wards. Severity assessment scores (CURB-65, PSI, APACHE II, SOFA) and serologic markers (HMGB-1, RAGE, sRAGE) were evaluated on admission.
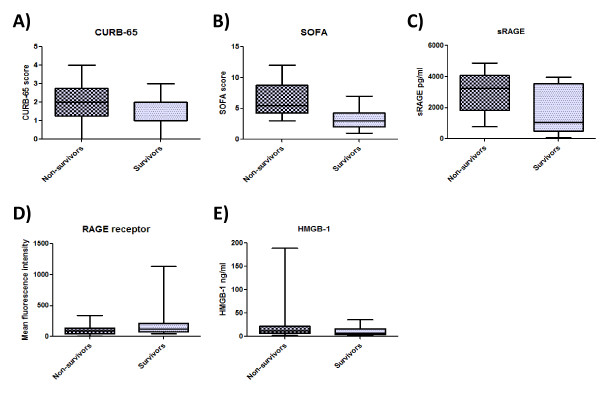
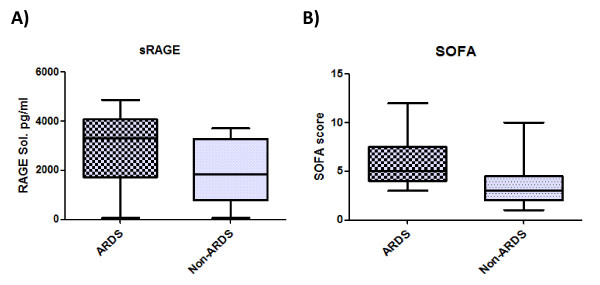
Thirty patients with a diagnosis of CAP-associated sepsis were enrolled in the study within 24 hours after admission. Fourteen (46.6%) had pandemic (H1N1) influenza A virus, 2 (6.6%) had seasonal influenza A and 14 other diagnoses. Of the patients in the study group, 16 (53.3%) had a fatal outcome. ARDS was observed in 17 (56.6%) and a total of 22 patients had severe sepsis on admission (73%). The SOFA score showed the greatest difference between surviving and non-surviving groups (P = .003) with similar results in ARDS patients (P = .005). sRAGE levels tended to be higher in non-surviving (P = .058) and ARDS patients (P = .058). Logistic regression modeling demonstrated that SOFA (P = .013) and sRAGE (P = .05) were the only variables that modified the probability of a fatal outcome.
The association of elevated sRAGE with a fatal outcome suggests that it may have an independent causal effect in CAP. SOFA scores were the only clinical factor with the ability to identify surviving and ARDS patients.
社区获得性肺炎(CAP)被认为是发达国家中传染性疾病导致死亡的最重要原因。严重程度评估评分部分解决了识别高危患者的困难。缺乏特异性和有效的病理生理学严重程度标志物会影响早期和有效的脓毒症治疗。HMGB-1、sRAGE 和 RAGE 参与了脓毒症,并且它们作为严重程度标志物的潜力已经被提出。本研究的目的是评估 CAP 相关脓毒症患者的 HMGB-1、RAGE 和 sRAGE 水平,并确定它们与临床结局的可能关联。
我们评估了 33 例因 CAP 相关脓毒症而收入急诊室并在医疗病房接受随访的患者。在入院时评估了严重程度评估评分(CURB-65、PSI、APACHE II、SOFA)和血清标志物(HMGB-1、RAGE、sRAGE)。
在入院后 24 小时内,我们招募了 30 例 CAP 相关脓毒症患者入组本研究。其中 14 例(46.6%)患有大流行(H1N1)流感 A 病毒,2 例(6.6%)患有季节性流感 A 病毒,其余 14 例为其他诊断。在研究组中,有 16 例(53.3%)患者死亡。ARDS 见于 17 例(56.6%)患者,入院时共有 22 例患者患有严重脓毒症(73%)。SOFA 评分在存活组和非存活组之间差异最大(P =.003),ARDS 患者的结果相似(P =.005)。sRAGE 水平在非存活组(P =.058)和 ARDS 患者中(P =.058)有升高趋势。Logistic 回归模型表明,SOFA(P =.013)和 sRAGE(P =.05)是唯一改变病死率的变量。
sRAGE 升高与死亡结局相关,这表明它可能在 CAP 中具有独立的因果作用。SOFA 评分是唯一具有识别存活和 ARDS 患者能力的临床因素。