Department of Infectious Diseases, Barwon Health, Geelong, Australia.
PLoS Negl Trop Dis. 2012 Jan;6(1):e1473. doi: 10.1371/journal.pntd.0001473. Epub 2012 Jan 17.
The World Health Organization currently recommends combined streptomycin and rifampicin antibiotic treatment as first-line therapy for Mycobacterium ulcerans infections. Alternatives are needed when these are not tolerated or accepted by patients, contraindicated, or neither accessible nor affordable. Despite in vitro effectiveness, clinical evidence for fluoroquinolone antibiotic use against Mycobacterium ulcerans is lacking. We describe outcomes and tolerability of fluoroquinolone-containing antibiotic regimens for Mycobacterium ulcerans in south-eastern Australia.
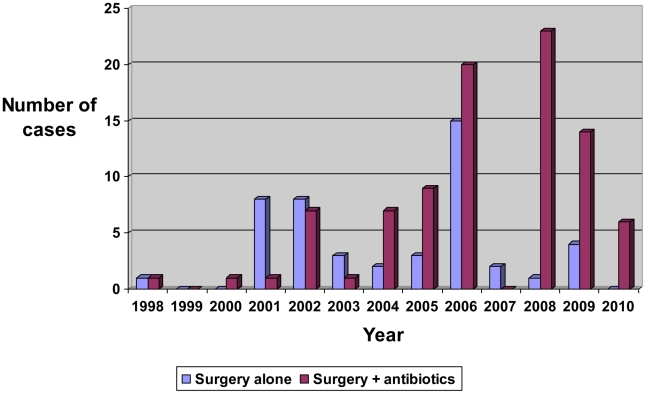
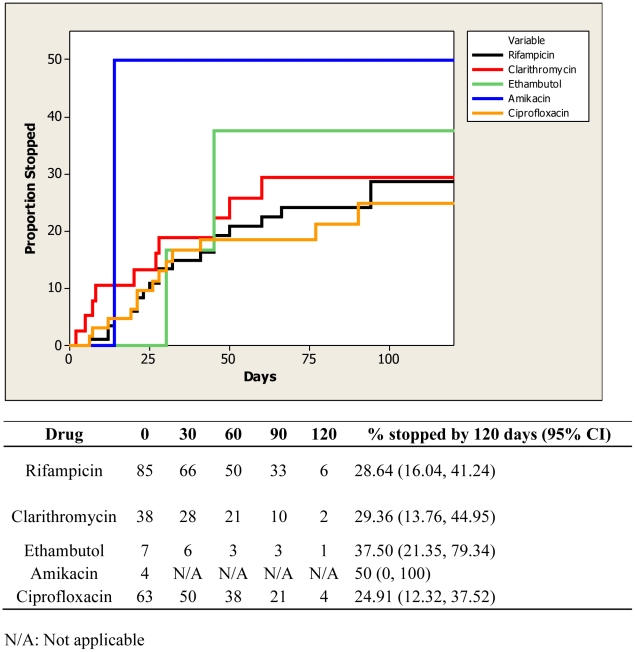
METHODOLOGY/PRINCIPAL FINDINGS: Analysis was performed of prospectively collected data including all primary Mycobacterium ulcerans infections treated at Barwon Health between 1998 and 2010. Medical treatment involved antibiotic use for more than 7 days; surgical treatment involved surgical excision of a lesion. Treatment success was defined as complete lesion healing without recurrence at 12 months follow-up. A complication was defined as an adverse event attributed to an antibiotic that required its cessation. A total of 133 patients with 137 lesions were studied. Median age was 62 years (range 3-94 years). 47 (34%) had surgical treatment alone, and 90 (66%) had combined surgical and medical treatment. Rifampicin and ciprofloxacin comprised 61% and rifampicin and clarithromycin 23% of first-line antibiotic regimens. 13/47 (30%) treated with surgery alone failed treatment compared to 0/90 (0%) of those treated with combination medical and surgical treatment (p<0.0001). There was no difference in treatment success rate for antibiotic combinations containing a fluoroquinolone (61/61 cases; 100%) compared with those not containing a fluoroquinolone (29/29 cases; 100%). Complication rates were similar between ciprofloxacin and rifampicin (31%) and rifampicin and clarithromycin (33%) regimens (OR 0.89, 95% CI 0.27-2.99). Paradoxical reactions during treatment were observed in 8 (9%) of antibiotic treated cases.
Antibiotics combined with surgery may significantly increase treatment success for Mycobacterium ulcerans infections, and fluoroquinolone combined with rifampicin-containing antibiotic regimens can provide an effective and safe oral treatment option.
世界卫生组织目前推荐将链霉素和利福平联合抗生素治疗作为治疗溃疡分枝杆菌感染的一线疗法。当这些治疗方法不能被患者耐受或接受、有禁忌症、无法获得或负担不起时,就需要替代方法。尽管氟喹诺酮类抗生素在体外具有有效性,但缺乏针对溃疡分枝杆菌的临床证据。我们描述了在澳大利亚东南部使用含氟喹诺酮类抗生素治疗溃疡分枝杆菌的结果和耐受性。
方法/主要发现:对 1998 年至 2010 年期间在巴旺健康中心治疗的所有原发性溃疡分枝杆菌感染进行了前瞻性收集数据的分析。医疗治疗包括抗生素治疗超过 7 天;手术治疗包括病变切除。治疗成功定义为 12 个月随访时完全愈合且无复发。并发症定义为归因于抗生素的不良事件,需要停止使用抗生素。共研究了 133 例患者的 137 处病变。中位年龄为 62 岁(范围 3-94 岁)。47 例(34%)单独接受手术治疗,90 例(66%)接受手术联合药物治疗。利福平加环丙沙星占一线抗生素方案的 61%,利福平加克拉霉素占 23%。单独手术治疗的 47 例中有 13 例(30%)治疗失败,而联合手术和药物治疗的 90 例中无一例(0%)(p<0.0001)。含氟喹诺酮类的抗生素联合治疗的成功率为 61/61 例(100%),与不含氟喹诺酮类的抗生素联合治疗的成功率为 29/29 例(100%),无差异。含氟喹诺酮类(31%)和不含氟喹诺酮类(33%)方案的环丙沙星和利福平的并发症发生率相似(OR 0.89,95%CI 0.27-2.99)。在接受抗生素治疗的病例中,观察到 8 例(9%)出现治疗期间的矛盾反应。
抗生素联合手术可能显著提高溃疡分枝杆菌感染的治疗成功率,氟喹诺酮类联合含利福平的抗生素方案可为有效的安全口服治疗选择。