London School of Hygiene and Tropical Medicine, London, United Kingdom.
PLoS One. 2012;7(1):e28957. doi: 10.1371/journal.pone.0028957. Epub 2012 Jan 31.
Antimalarial resistance has led to a global policy of artemisinin-based combination therapy. Despite growing resistance chloroquine (CQ) remained until recently the official first-line treatment for falciparum malaria in Pakistan, with sulfadoxine-pyrimethamine (SP) second-line. Co-treatment with the gametocytocidal primaquine (PQ) is recommended for transmission control in South Asia. The relative effect of artesunate (AS) or primaquine, as partner drugs, on clinical outcomes and gametocyte carriage in this setting were unknown.
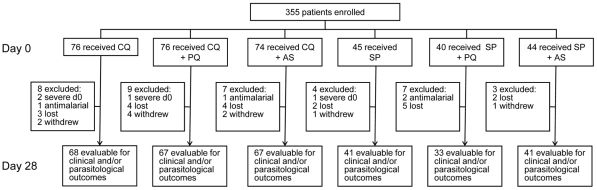
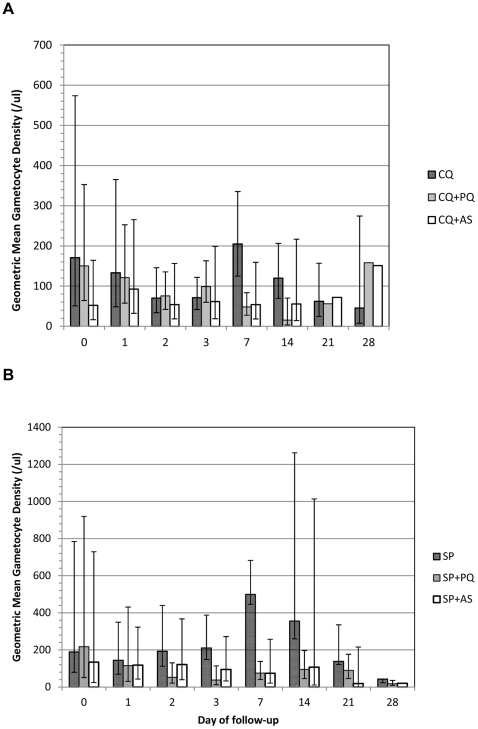
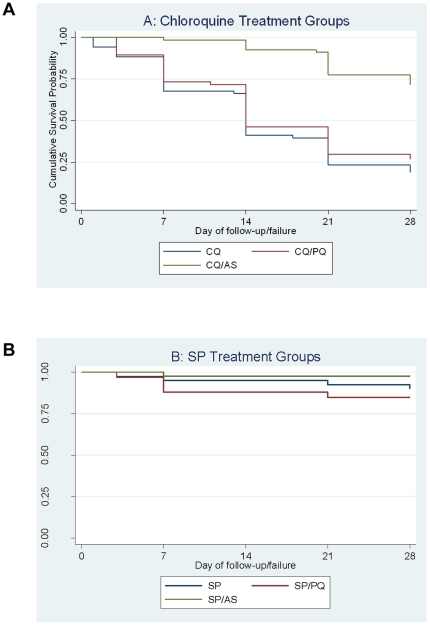
A single-blinded, randomized trial among Afghan refugees in Pakistan compared six treatment arms: CQ; CQ+(single-dose)PQ; CQ+(3 d)AS; SP; SP+(single-dose)PQ, and SP+(3 d)AS. The objectives were to compare treatment failure rates and effect on gametocyte carriage, of CQ or SP monotherapy against the respective combinations (PQ or AS). Outcomes included trophozoite and gametocyte clearance (read by light microscopy), and clinical and parasitological failure.
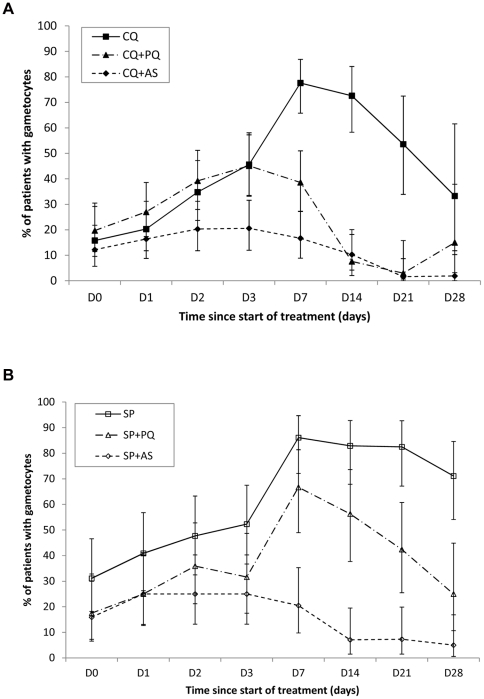
A total of 308 (87%) patients completed the trial. Failure rates by day 28 were: CQ 55/68 (81%); CQ+AS 19/67 (28%), SP 4/41 (9.8%), SP+AS 1/41 (2.4%). The addition of PQ to CQ or SP did not affect failure rates (CQ+PQ 49/67 (73%) failed; SP+PQ 5/33 (16%) failed). AS was superior to PQ at clearing gametocytes; gametocytes were seen on d7 in 85% of CQ, 40% of CQ+PQ, 21% of CQ+AS, 91% of SP, 76% of SP+PQ and 23% of SP+AS treated patients. PQ was more effective at clearing older gametocyte infections whereas AS was more effective at preventing emergence of mature gametocytes, except in cases that recrudesced.
CQ is no longer appropriate by itself or in combination. These findings influenced the replacement of CQ with SP+AS for first-line treatment of uncomplicated falciparum malaria in the WHO Eastern Mediterranean Region. The threat of SP resistance remains as SP monotherapy is still common. Three day AS was superior to single-dose PQ for reducing gametocyte carriage.
ClinicalTrials.gov NCT00959517.
抗疟药物的耐药性导致了全球范围内使用青蒿素类药物联合疗法的政策。尽管氯喹(CQ)的耐药性不断增加,但直到最近,它仍是巴基斯坦恶性疟原虫的官方一线治疗药物,而磺胺多辛-乙胺嘧啶(SP)是二线药物。在南亚,建议联合使用配子体杀灭剂伯氨喹(PQ)来控制传播。在这种情况下,青蒿琥酯(AS)或伯氨喹作为联合用药对临床结局和配子体携带的相对影响尚不清楚。
在巴基斯坦的阿富汗难民中进行了一项单盲、随机试验,比较了六种治疗方案:CQ;CQ+(单剂量)PQ;CQ+(3d)AS;SP;SP+(单剂量)PQ 和 SP+(3d)AS。目的是比较 CQ 或 SP 单药治疗与各自联合用药(PQ 或 AS)的治疗失败率和配子体携带情况。结果包括滋养体和配子体清除(通过光学显微镜读取)以及临床和寄生虫学失败。
共有 308 名(87%)患者完成了试验。第 28 天的失败率为:CQ 55/68(81%);CQ+AS 19/67(28%),SP 4/41(9.8%),SP+AS 1/41(2.4%)。在 CQ 或 SP 中添加 PQ 并没有影响失败率(CQ+PQ 49/67(73%)失败;SP+PQ 5/33(16%)失败)。AS 在清除配子体方面优于 PQ;在接受治疗的患者中,第 7 天仍可见 CQ 的配子体 85%,CQ+PQ 的 40%,CQ+AS 的 21%,SP 的 91%,SP+PQ 的 76%,SP+AS 的 23%。PQ 更有效地清除陈旧的配子体感染,而 AS 更有效地防止成熟配子体的出现,除非发生复发。
CQ 本身或联合用药已不再适用。这些发现影响了世卫组织东地中海区域将 CQ 用 SP+AS 取代用于治疗无并发症恶性疟原虫的一线药物。SP 单药治疗仍然很常见,因此 SP 耐药性的威胁仍然存在。3 天 AS 优于单剂量 PQ,可降低配子体携带率。
ClinicalTrials.gov NCT00959517。