General Practice and Primary Care, Institute of Health and Wellbeing, University of Glasgow, 1 Horselethill Road, Glasgow, UK.
BMC Fam Pract. 2012 Feb 8;13:6. doi: 10.1186/1471-2296-13-6.
Patient 'enablement' is a term closely aligned with 'empowerment' and its measurement in a general practice consultation has been operationalised in the widely used patient enablement instrument (PEI), a patient-rated measure of consultation outcome. However, there is limited knowledge regarding the factors that influence enablement, particularly the effect of socio-economic deprivation. The aim of the study is to assess the factors influencing patient enablement in GP consultations in areas of high and low deprivation.
A questionnaire study was carried out on 3,044 patients attending 26 GPs (16 in areas of high socio-economic deprivation and 10 in low deprivation areas, in the west of Scotland). Patient expectation (confidence that the doctor would be able to help) was recorded prior to the consultation. PEI, GP empathy (measured by the CARE Measure), and a range of other measures and variables were recorded after the consultation. Data analysis employed multi-level modelling and multivariate analyses with the PEI as the dependant variable.
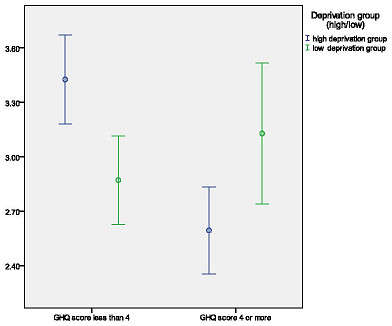
Although numerous variables showed a univariate association with patient enablement, only four factors were independently predictive after multilevel multivariate analysis; patients with multimorbidity of 3 or more long-term conditions (reflecting poor chronic general health), and those consulting about a long-standing problem had reduced enablement scores in both affluent and deprived areas. In deprived areas, emotional distress (GHQ-caseness) had an additional negative effect on enablement. Perceived GP empathy had a positive effect on enablement in both affluent and deprived areas. Maximal patient enablement was never found with low empathy.
Although other factors influence patient enablement, the patients' perceptions of the doctors' empathy is of key importance in patient enablement in general practice consultations in both high and low deprivation settings.
患者“赋权”是一个与“授权”密切相关的术语,其在一般实践咨询中的衡量标准已在广泛使用的患者赋权工具(PEI)中实现,这是一种衡量咨询结果的患者自评工具。然而,关于影响赋权的因素,特别是社会经济贫困的影响,知之甚少。本研究旨在评估在高贫困和低贫困地区的全科医生咨询中影响患者赋权的因素。
对 3044 名在 26 名全科医生(16 名在社会经济贫困地区,10 名在贫困地区,苏格兰西部)就诊的患者进行了问卷调查。在咨询前记录了患者的期望(对医生能够提供帮助的信心)。在咨询后记录了 PEI、全科医生共情(通过 CARE 量表测量)以及其他一系列措施和变量。数据分析采用多水平模型和多元分析,以 PEI 为因变量。
尽管许多变量在单变量分析中与患者赋权相关,但只有四个因素在多水平多元分析后具有独立性预测作用;患有 3 种或以上长期疾病的患者(反映慢性一般健康状况不佳)和长期存在问题的患者,在富裕和贫困地区的赋权评分都较低。在贫困地区,情绪困扰(GHQ 发病)对赋权产生额外的负面影响。患者感知的全科医生共情对富裕和贫困地区的赋权都有积极影响。在共情程度低的情况下,患者的赋权程度从未达到最高。
尽管其他因素也会影响患者的赋权,但患者对医生共情的感知在高贫困和低贫困环境下的全科医生咨询中对患者赋权至关重要。