Aaron Diamond AIDS Research Center, New York, New York, USA.
PLoS Pathog. 2012 Feb;8(2):e1002506. doi: 10.1371/journal.ppat.1002506. Epub 2012 Feb 2.
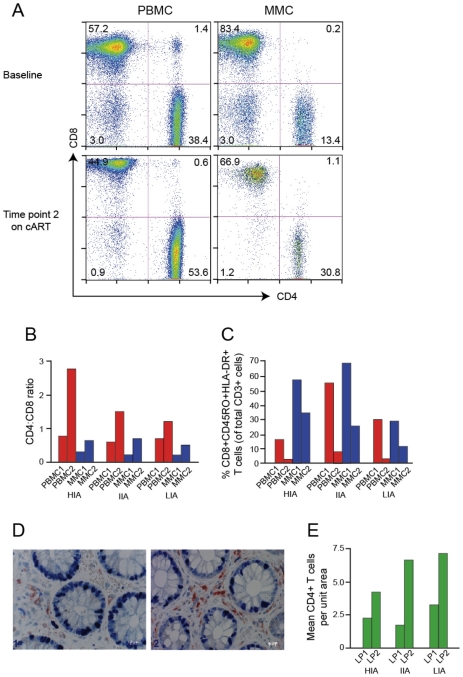
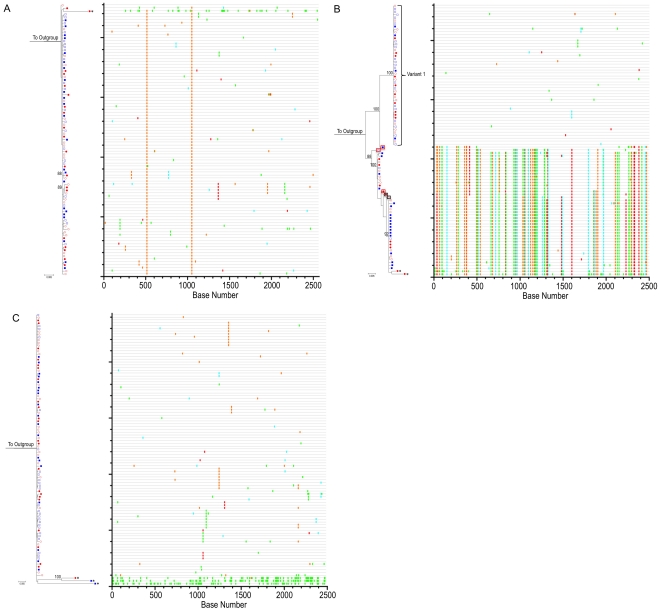
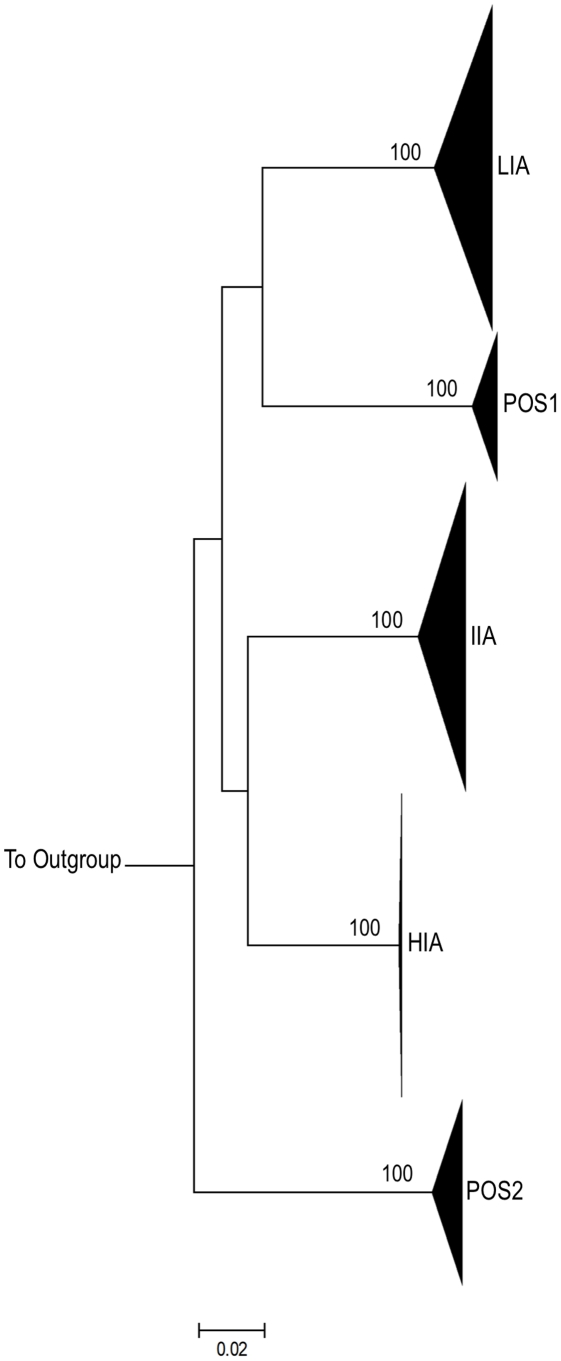
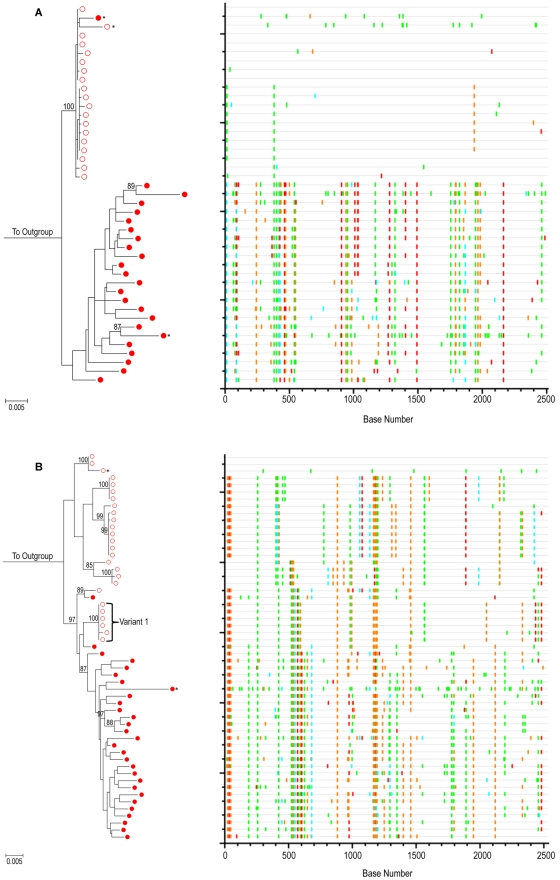
Mucosal mononuclear (MMC) CCR5+CD4+ T cells of the gastrointestinal (GI) tract are selectively infected and depleted during acute HIV-1 infection. Despite early initiation of combination antiretroviral therapy (cART), gut-associated lymphoid tissue (GALT) CD4+ T cell depletion and activation persist in the majority of HIV-1 positive individuals studied. This may result from ongoing HIV-1 replication and T-cell activation despite effective cART. We hypothesized that ongoing viral replication in the GI tract during cART would result in measurable viral evolution, with divergent populations emerging over time. Subjects treated during early HIV-1 infection underwent phlebotomy and flexible sigmoidoscopy with biopsies prior to and 15-24 months post initiation of cART. At the 2(nd) biopsy, three GALT phenotypes were noted, characterized by high, intermediate and low levels of immune activation. A representative case from each phenotype was analyzed. Each subject had plasma HIV-1 RNA levels <50 copies/ml at 2(nd) GI biopsy and CD4+ T cell reconstitution in the peripheral blood. Single genome amplification of full-length HIV-1 envelope was performed for each subject pre- and post-initiation of cART in GALT and PBMC. A total of 280 confirmed single genome sequences (SGS) were analyzed for experimental cases. For each subject, maximum likelihood phylogenetic trees derived from molecular sequence data showed no evidence of evolved forms in the GALT over the study period. During treatment, HIV-1 envelope diversity in GALT-derived SGS did not increase and post-treatment GALT-derived SGS showed no substantial genetic divergence from pre-treatment sequences within transmitted groups. Similar results were obtained from PBMC-derived SGS. Our results reveal that initiation of cART during acute/early HIV-1 infection can result in the interruption of measurable viral evolution in the GALT, suggesting the absence of de-novo rounds of HIV-1 replication in this compartment during suppressive cART.
胃肠道(GI)黏膜单核(MMC)CCR5+CD4+T 细胞在急性 HIV-1 感染期间会被选择性感染和耗竭。尽管早期开始联合抗逆转录病毒治疗(cART),但在大多数研究的 HIV-1 阳性个体中,肠道相关淋巴组织(GALT)CD4+T 细胞耗竭和激活仍然存在。这可能是由于尽管 cART 有效,但 HIV-1 复制和 T 细胞激活仍在持续。我们假设,在 cART 期间,胃肠道内持续的病毒复制会导致可测量的病毒进化,随着时间的推移,会出现不同的病毒群体。在 HIV-1 早期感染期间接受治疗的受试者在开始 cART 前和 15-24 个月后进行了静脉采血和乙状结肠镜检查和活检。在第二次活检中,观察到三种 GALT 表型,其特征为免疫激活水平高、中、低。对每种表型的一个代表性病例进行了分析。每个受试者在第二次 GI 活检时血浆 HIV-1 RNA 水平<50 拷贝/ml,外周血中 CD4+T 细胞重建。对每位受试者在 GALT 和 PBMC 中 cART 开始前后进行全长 HIV-1 包膜的单基因组扩增。对 280 个经证实的单基因组序列(SGS)进行了分析。对于每个受试者,从分子序列数据得出的最大似然系统发育树显示,在研究期间,GALT 中没有进化形式的证据。在治疗期间,GALT 衍生 SGS 中的 HIV-1 包膜多样性没有增加,治疗后 GALT 衍生 SGS 与传播组内治疗前序列相比没有明显的遗传差异。从 PBMC 衍生的 SGS 中也得到了类似的结果。我们的研究结果表明,在急性/早期 HIV-1 感染期间开始 cART 可导致 GALT 中可测量的病毒进化中断,表明在抑制性 cART 期间,该部位不存在新的 HIV-1 复制循环。