Massachusetts General Hospital and Ragon Institute, Boston, Massachusetts, United States of America.
PLoS Med. 2010 Aug 10;7(8):e1000321. doi: 10.1371/journal.pmed.1000321.
Most HIV-1-infected patients on effective antiretroviral therapy (ART) with plasma HIV-1 RNA levels below the detection limits of commercial assays have residual viremia measurable by more sensitive methods. We assessed whether adding raltegravir lowered the level of residual viremia in such patients.
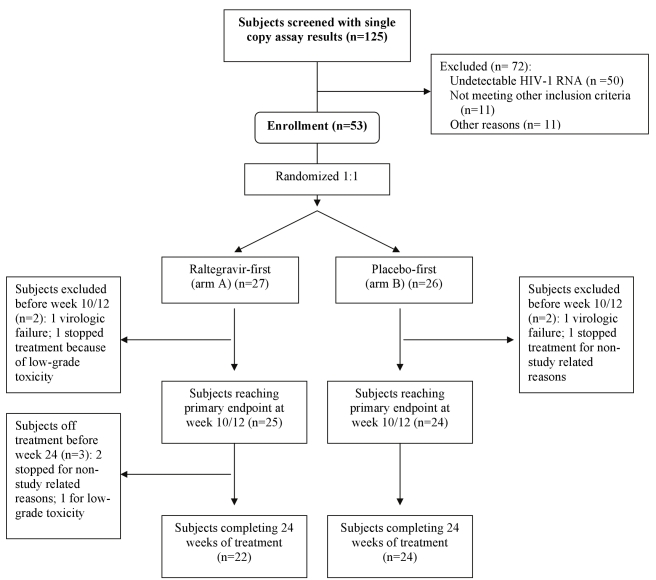
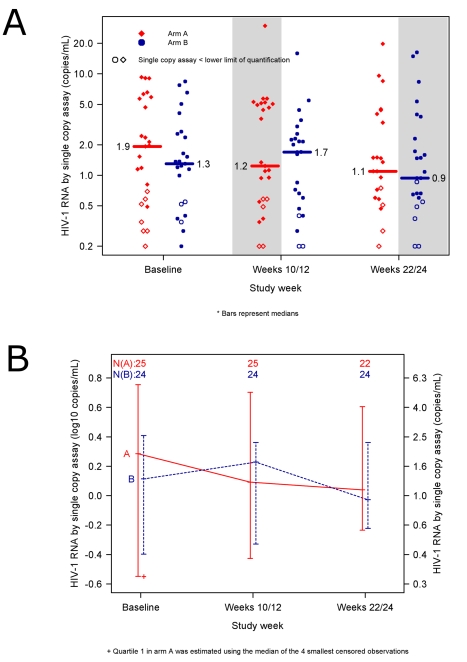
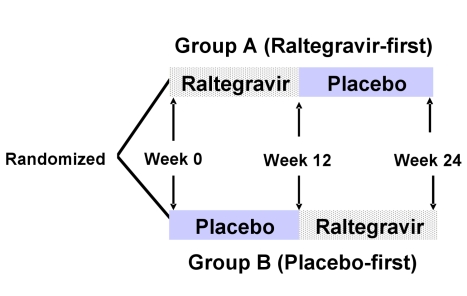
Patients receiving ART who had plasma HIV-1 RNA levels below 50 copies/mL but detectable viremia by single copy assay (SCA) were randomized to add either raltegravir or placebo to their ART regimen for 12 weeks; patients then crossed-over to the other therapy for an additional 12 weeks while continuing pre-study ART. The primary endpoint was the plasma HIV-1 RNA by SCA averaged between weeks 10 and 12 (10/12) compared between treatment groups. Fifty-three patients were enrolled. The median screening HIV-1 RNA was 1.7 copies/mL. The HIV-1 RNA level at weeks 10/12 did not differ significantly between the raltegravir-intensified (n = 25) and the placebo (n = 24) groups (median 1.2 versus 1.7 copies/mL, p = 0.55, Wilcoxon rank sum test), nor did the change in HIV-1 RNA level from baseline to week 10/12 (median -0.2 and -0.1 copies/mL, p = 0.71, Wilcoxon rank sum test). There was also no significant change in HIV-1 RNA level from weeks 10/12 to weeks 22/24 after patients crossed-over. There was a greater CD4 cell count increase from baseline to week 12 in the raltegravir-intensified group compared with the placebo group (+42 versus -44 cells/mm(3), p = 0.082, Wilcoxon rank sum test), which reversed after the cross-over. This CD4 cell count change was not associated with an effect of raltegravir intensification on markers of CD4 or CD8 cell activation in blood.
In this randomized, double-blind cross-over study, 12 weeks of raltegravir intensification did not demonstrably reduce low-level plasma viremia in patients on currently recommended ART. This finding suggests that residual viremia does not arise from ongoing cycles of HIV-1 replication and infection of new cells. New therapeutic strategies to eliminate reservoirs that produce residual viremia will be required to eradicate HIV-1 infection.
ClinicalTrials.gov NCT00515827
大多数接受高效抗逆转录病毒治疗(ART)且血浆 HIV-1 RNA 水平低于商业检测下限的 HIV-1 感染患者,采用更敏感的方法可检测到残留的病毒血症。我们评估了加用拉替拉韦是否可降低此类患者的残留病毒血症水平。
接受 ART 治疗且血浆 HIV-1 RNA 水平低于 50 拷贝/ml,但单拷贝检测法(SCA)可检测到病毒血症的患者被随机分配至在 ART 方案中加用拉替拉韦或安慰剂治疗 12 周;然后患者交叉换用另一种治疗方案,再接受 12 周的治疗,同时继续接受预研究的 ART。主要终点是治疗组间 10-12 周时 SCA 平均 HIV-1 RNA(10/12)。共纳入 53 例患者。筛查时的中位 HIV-1 RNA 为 1.7 拷贝/ml。拉替拉韦强化治疗组(n = 25)和安慰剂组(n = 24)在 10/12 周时 HIV-1 RNA 水平无显著差异(中位数分别为 1.2 和 1.7 拷贝/ml,p = 0.55,Wilcoxon 秩和检验),HIV-1 RNA 水平从基线到 10/12 周的变化也无显著差异(中位数分别为-0.2 和-0.1 拷贝/ml,p = 0.71,Wilcoxon 秩和检验)。患者交叉换用后,10/12 周至 22/24 周时 HIV-1 RNA 水平也无显著变化。与安慰剂组相比,拉替拉韦强化组在第 12 周时 CD4 细胞计数从基线的增加更明显(+42 与-44 个细胞/mm3,p = 0.082,Wilcoxon 秩和检验),交叉换用后这种变化逆转。这种 CD4 细胞计数的变化与拉替拉韦强化对血液中 CD4 或 CD8 细胞激活标志物的作用无关。
在这项随机、双盲交叉研究中,12 周的拉替拉韦强化治疗并未显著降低正在接受推荐的 ART 治疗的患者的低水平血浆病毒血症。这一发现表明,残留病毒血症不是由 HIV-1 复制和感染新细胞的持续循环引起的。需要新的治疗策略来消除产生残留病毒血症的储库,以消灭 HIV-1 感染。
ClinicalTrials.gov NCT00515827