Department of Biostatistics and Computational Biology, Dana-Farber Cancer Institute, Boston, MA 02215, USA.
Clin Trials. 2012 Apr;9(2):155-63. doi: 10.1177/1740774512436614. Epub 2012 Feb 21.
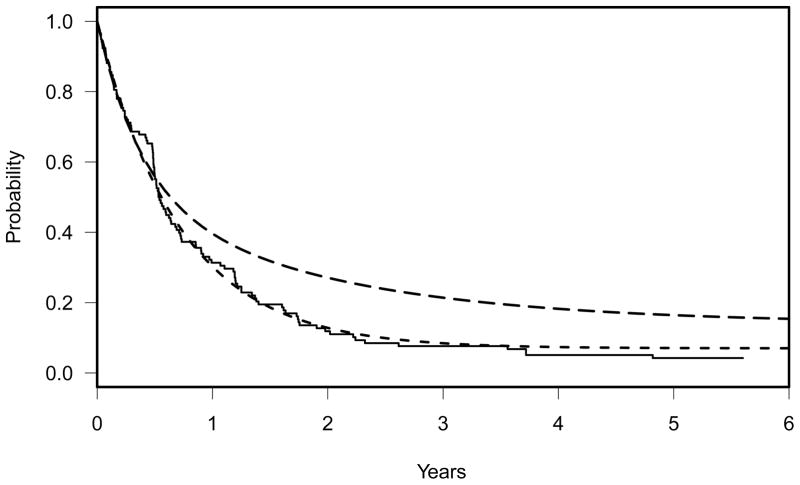
Cure rate models have been extensively studied and widely used in time-to-event data in cancer clinical trials.
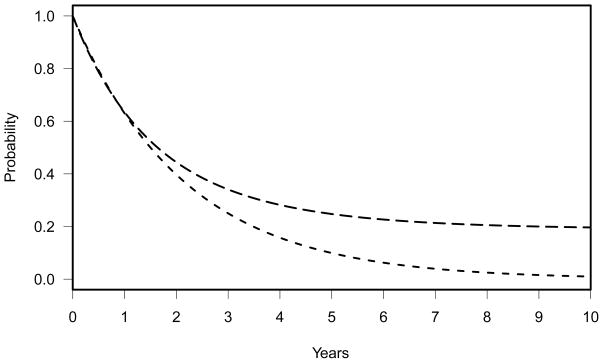
Although cure rate models based on the generalized exponential distribution have been developed, they have not been used in the design of randomized cancer clinical trials, which instead have relied exclusively on two-component exponential cure rate model with a proportional hazards (PH) alternative. In some studies, the efficacy of the experimental treatment is expected to emerge some time after randomization. Since this does not conform to a PH alternative, such studies require a more flexible model to describe the alternative hypothesis.
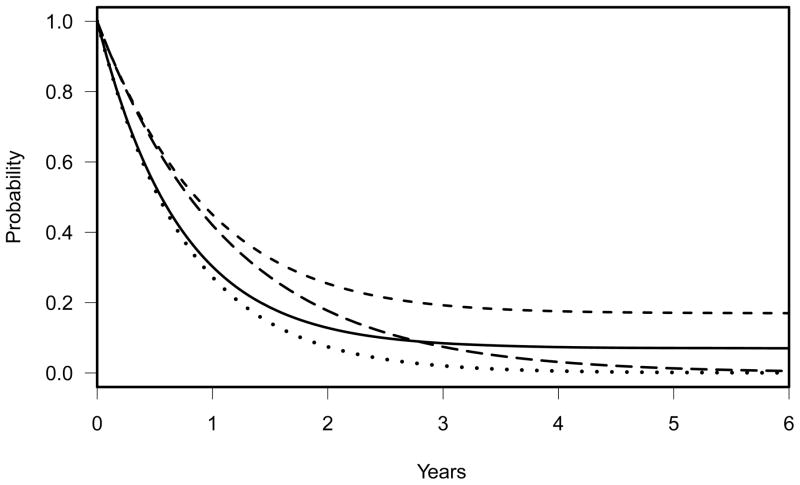
In this article, we report the study design of a phase III clinical trial of acute myeloid leukemia using a three-component exponential cure rate model to reflect the alternative hypothesis. A newly developed power calculation program that does not require PH assumption was used.
Using a custom-made three-component cure rate model as an alternative hypothesis, the proposed sample size was 409, compared with a sample size of 209 under the assumption of exponential distribution and 228 under the PH alternative. A simulation study was performed to present the degree of power loss when the alternative hypothesis is not appropriately specified.
The power calculation program used in this study is for a single analysis and does not account for group sequential tests in phase III trials. However, the loss in power is small, and this was handled by inflating the sample size by 5%.
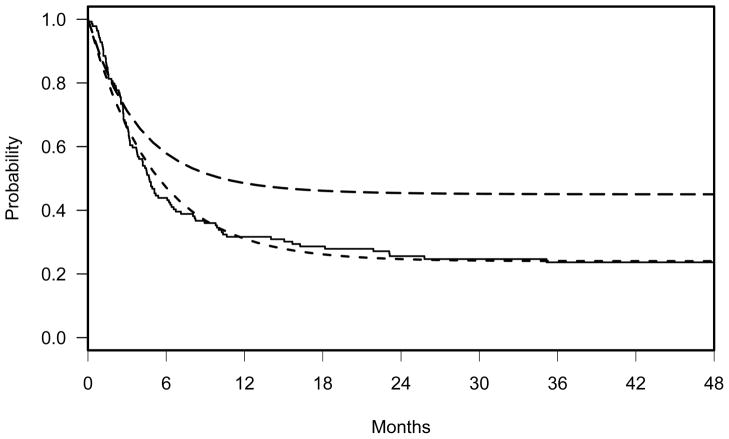
Misspecification of the alternative hypothesis can result in a seriously underpowered study. We report examples of clinical trials that required a custom-made alternative hypothesis to reflect a later indication of experimental treatment efficacy. The proposed three-component cure rate model could be very useful for specifying non-PH alternative.
在癌症临床试验的时间事件数据中,已经广泛研究和应用了治愈率模型。
尽管已经开发了基于广义指数分布的治愈率模型,但它们并未在随机癌症临床试验的设计中得到应用,而是完全依赖于具有比例风险(PH)替代方案的两成分指数治愈率模型。在某些研究中,实验治疗的疗效预计会在随机化后一段时间出现。由于这不符合 PH 替代方案,因此此类研究需要更灵活的模型来描述替代假设。
在本文中,我们报告了使用三成分指数治愈率模型来反映替代假设的急性髓细胞白血病 III 期临床试验的研究设计。使用了一种新开发的无需 PH 假设的功效计算程序。
使用定制的三成分治愈率模型作为替代假设,建议的样本量为 409 例,而指数分布假设下的样本量为 209 例,PH 替代方案下的样本量为 228 例。进行了模拟研究,以展示替代假设不适当指定时的功效损失程度。
本研究中使用的功效计算程序仅适用于单一分析,并未考虑 III 期试验中的分组序贯检验。但是,功效损失很小,这可以通过将样本量增加 5%来处理。
替代假设的不正确指定可能导致研究严重功效不足。我们报告了一些临床试验的例子,这些临床试验需要定制的替代假设来反映实验治疗疗效的后期迹象。所提出的三成分治愈率模型对于指定非 PH 替代方案非常有用。