Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women's Hospital and Harvard Medical School, Boston, 02120 MA, United States.
BMJ. 2012 Feb 23;344:e977. doi: 10.1136/bmj.e977.
To assess risks of mortality associated with use of individual antipsychotic drugs in elderly residents in nursing homes.
Population based cohort study with linked data from Medicaid, Medicare, the Minimum Data Set, the National Death Index, and a national assessment of nursing home quality.
Nursing homes in the United States.
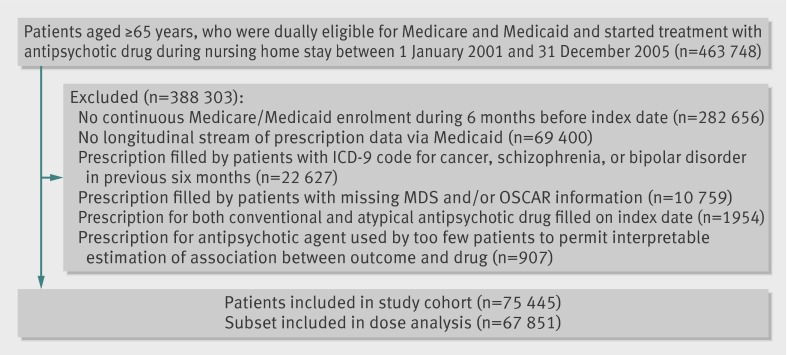
75,445 new users of antipsychotic drugs (haloperidol, aripiprazole, olanzapine, quetiapine, risperidone, ziprasidone). All participants were aged ≥ 65, were eligible for Medicaid, and lived in a nursing home in 2001-5.
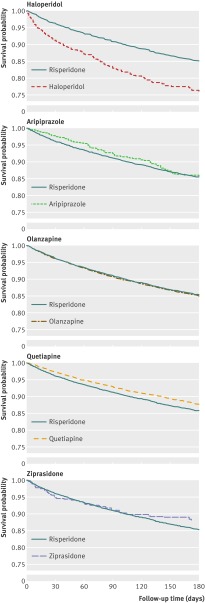
Cox proportional hazards models were used to compare 180 day risks of all cause and cause specific mortality by individual drug, with propensity score adjustment to control for potential confounders.
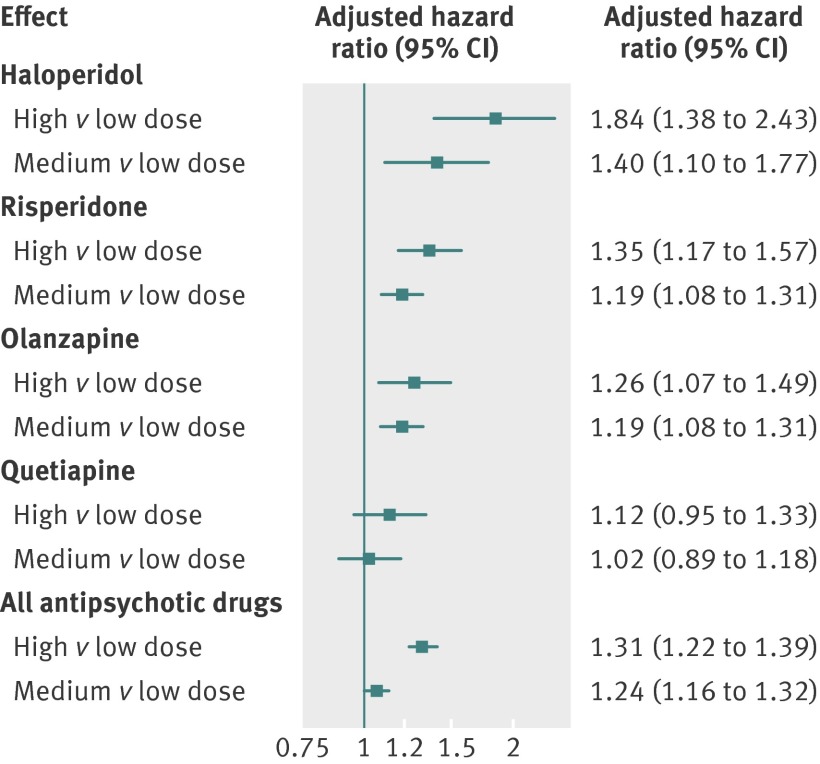
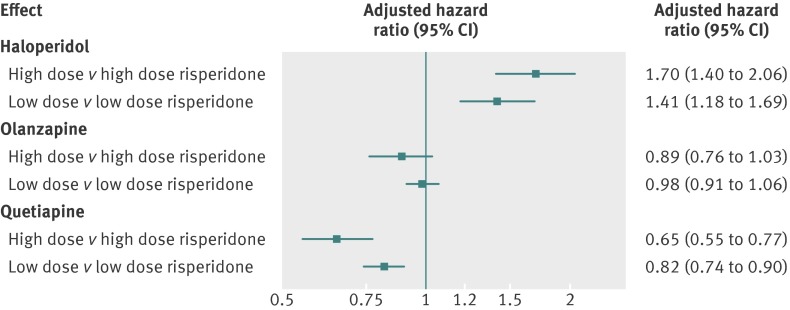
Compared with risperidone, users of haloperidol had an increased risk of mortality (hazard ratio 2.07, 95% confidence interval 1.89 to 2.26) and users of quetiapine a decreased risk (0.81, 0.75 to 0.88). The effects were strongest shortly after the start of treatment, remained after adjustment for dose, and were seen for all causes of death examined. No clinically meaningful differences were observed for the other drugs. There was no evidence that the effect measure modification in those with dementia or behavioural disturbances. There was a dose-response relation for all drugs except quetiapine.
Though these findings cannot prove causality, and we cannot rule out the possibility of residual confounding, they provide more evidence of the risk of using these drugs in older patients, reinforcing the concept that they should not be used in the absence of clear need. The data suggest that the risk of mortality with these drugs is generally increased with higher doses and seems to be highest for haloperidol and least for quetiapine.
评估在养老院的老年居民中使用个别抗精神病药物与死亡率相关的风险。
基于人群的队列研究,数据来自医疗补助计划、医疗保险、最低数据集合、国家死亡索引和全国养老院质量评估。
美国养老院。
75445 名新使用抗精神病药物(氟哌啶醇、阿立哌唑、奥氮平、喹硫平、利培酮、齐拉西酮)的患者。所有参与者年龄均≥65 岁,有资格参加医疗补助计划,且于 2001-2005 年居住在养老院。
使用 Cox 比例风险模型比较每种药物在 180 天内的全因死亡率和特定原因死亡率的风险,通过倾向评分调整控制潜在混杂因素。
与利培酮相比,氟哌啶醇使用者的死亡率风险增加(风险比 2.07,95%置信区间 1.89 至 2.26),而喹硫平使用者的死亡率风险降低(0.81,0.75 至 0.88)。这种影响在治疗开始后不久最为强烈,在调整剂量后仍然存在,并且在所有研究的死亡原因中都存在。对于其他药物,没有观察到明显的临床意义上的差异。在痴呆或行为障碍患者中,没有证据表明药物效果的变化。除了喹硫平,所有药物都存在剂量-反应关系。
尽管这些发现不能证明因果关系,并且我们不能排除残留混杂的可能性,但它们为这些药物在老年患者中的使用风险提供了更多证据,强化了在缺乏明确需要的情况下不应使用这些药物的概念。数据表明,这些药物的死亡率风险通常随着剂量的增加而增加,氟哌啶醇的风险最高,喹硫平的风险最低。