Department of Internal Medicine, Villarrobledo Hospital, Villarrobledo, Spain.
PLoS One. 2012;7(2):e32090. doi: 10.1371/journal.pone.0032090. Epub 2012 Feb 29.
Brucellosis is a persistent health problem in many developing countries throughout the world, and the search for simple and effective treatment continues to be of great importance.
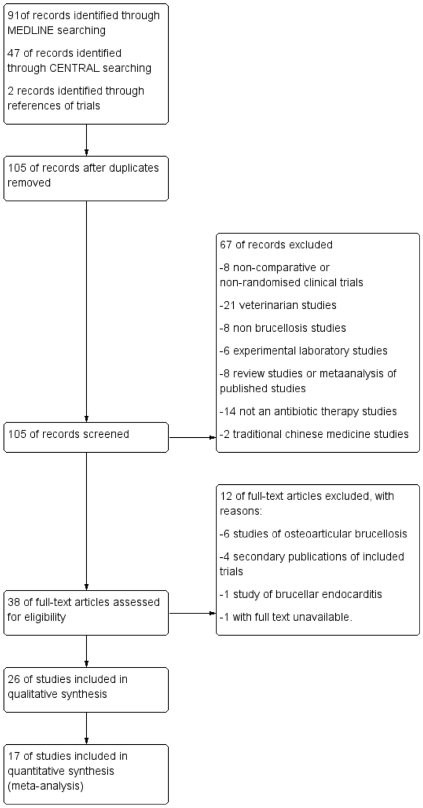
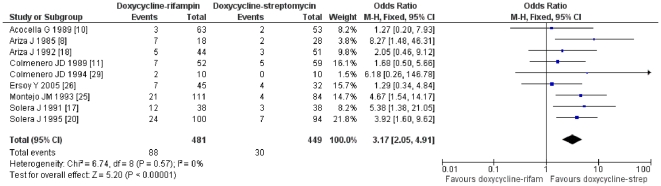
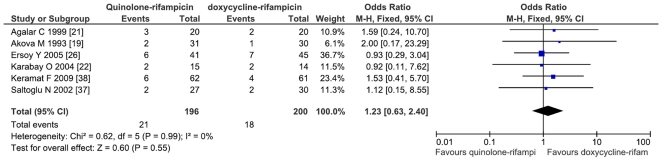
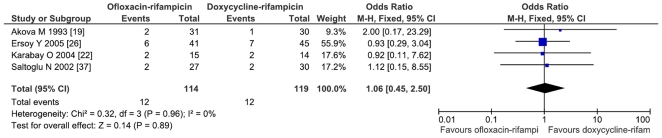
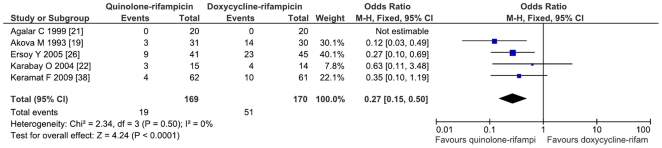
A search was conducted in MEDLINE and in the Cochrane Central Register of Controlled Trials (CENTRAL). Clinical trials published from 1985 to present that assess different antimicrobial regimens in cases of documented acute uncomplicated human brucellosis were included. The primary outcomes were relapse, therapeutic failure, combined variable of relapse and therapeutic failure, and adverse effect rates. A meta-analysis with a fixed effect model was performed and odds ratio with 95% confidence intervals were calculated. A random effect model was used when significant heterogeneity between studies was verified. Comparison of combined doxycycline and rifampicin with a combination of doxycycline and streptomycin favors the latter regimen (OR = 3.17; CI95% = 2.05-4.91). There were no significant differences between combined doxycycline-streptomycin and combined doxycycline-gentamicin (OR = 1.89; CI95% = 0.81-4.39). Treatment with rifampicin and quinolones was similar to combined doxycycline-rifampicin (OR = 1.23; CI95% = 0.63-2.40). Only one study assessed triple therapy with aminoglycoside-doxycycline-rifampicin and only included patients with uncomplicated brucellosis. Thus this approach cannot be considered the therapy of choice until further studies have been performed. Combined doxycycline/co-trimoxazole or doxycycline monotherapy could represent a cost-effective alternative in certain patient groups, and further studies are needed in the future.
Although the preferred treatment in uncomplicated human brucellosis is doxycycline-aminoglycoside combination, other treatments based on oral regimens or monotherapy should not be rejected until they are better studied. Triple therapy should not be considered the current treatment of choice.
布鲁氏菌病是世界上许多发展中国家持续存在的健康问题,寻找简单有效的治疗方法仍然非常重要。
在 MEDLINE 和 Cochrane 对照试验中心注册库(CENTRAL)中进行了检索。纳入了 1985 年至今发表的评估有明确记录的急性非复杂性人类布鲁氏菌病不同抗菌治疗方案的临床试验。主要结局为复发、治疗失败、复发和治疗失败的综合变量以及不良反应发生率。采用固定效应模型进行荟萃分析,并计算比值比及其 95%置信区间。当研究间存在显著异质性时,采用随机效应模型。比较多西环素和利福平联合与多西环素和链霉素联合,后者方案更优(OR=3.17;95%CI95%=2.05-4.91)。多西环素-链霉素联合与多西环素-庆大霉素联合(OR=1.89;95%CI95%=0.81-4.39)之间无显著差异。利福平与喹诺酮类药物联合与多西环素-利福平联合(OR=1.23;95%CI95%=0.63-2.40)相似。仅有一项研究评估了氨基糖苷类-多西环素-利福平三联疗法,且仅纳入了无并发症的布鲁氏菌病患者。因此,在进一步研究之前,不能将这种方法视为首选治疗方法。对于某些患者群体,多西环素/复方磺胺甲噁唑联合或多西环素单药治疗可能是一种具有成本效益的替代方法,未来需要进一步研究。
尽管在无并发症的人类布鲁氏菌病中,首选的治疗方法是多西环素-氨基糖苷类联合治疗,但在进一步研究之前,不应拒绝其他基于口服方案或单药治疗的治疗方法。三联疗法不应被视为当前的治疗选择。