Polizzotto Mark N, Uldrick Thomas S, Hu Duosha, Yarchoan Robert
HIV/AIDS Malignancy Branch, Center for Cancer Research, National Cancer Institute Bethesda, MD, USA.
Front Microbiol. 2012 Mar 2;3:73. doi: 10.3389/fmicb.2012.00073. eCollection 2012.
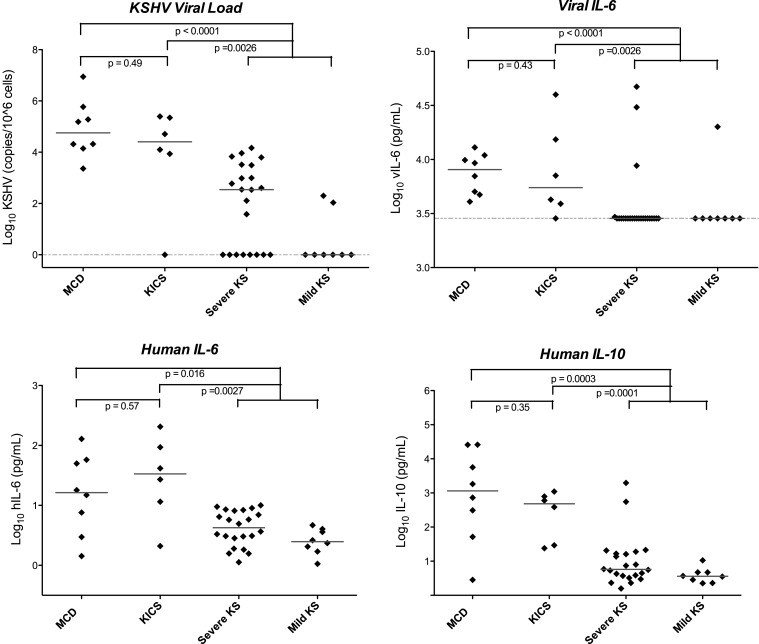
Soon after the discovery of Kaposi sarcoma (KS)-associated herpesvirus (KSHV), it was appreciated that this virus was associated with most cases of multicentric Castleman disease (MCD) arising in patients infected with human immunodeficiency virus. It has subsequently been recognized that KSHV-MCD is a distinct entity from other forms of MCD. Like MCD that is unrelated to KSHV, the clinical presentation of KSHV-MCD is dominated by systemic inflammatory symptoms including fevers, cachexia, and laboratory abnormalities including cytopenias, hypoalbuminemia, hyponatremia, and elevated C-reactive protein. Pathologically KSHV-MCD is characterized by polyclonal, IgM-lambda restricted plasmacytoid cells in the intrafollicular areas of affected lymph nodes. A portion of these cells are infected with KSHV and a sizable subset of these cells express KSHV lytic genes including a viral homolog of interleukin-6 (vIL-6). Patients with KSHV-MCD generally have elevated KSHV viral loads in their peripheral blood. Production of vIL-6 and induction of human (h) IL-6 both contribute to symptoms, perhaps in combination with overproduction of IL-10 and other cytokines. Until recently, the prognosis of patients with KSHV-MCD was poor. Recent therapeutic advances targeting KSHV-infected B cells with the anti-CD20 monoclonal antibody rituximab and utilizing KSHV enzymes to target KSHV-infected cells have substantially improved patient outcomes. Recently another KSHV-associated condition, the KSHV inflammatory cytokine syndrome (KICS) has been described. Its clinical manifestations resemble those of KSHV-MCD but lymphadenopathy is not prominent and the pathologic nodal changes of KSHV-MCD are absent. Patients with KICS exhibit elevated KSHV viral loads and elevation of vIL-6, homolog of human interleukin-6 and IL-10 comparable to those seen in KSHV-MCD; the cellular origin of these is a matter of investigation. KICS may contribute to the inflammatory symptoms seen in some patients with severe KS or primary effusion lymphoma. Additional research is needed to better define the clinical spectrum of KICS and its relationship to KSHV-MCD. In additional, research is needed to better understand the pathogenesis and epidemiology of both KICS and KSHV-MCD, as well as the optimal therapy for both of these disorders.
卡波西肉瘤相关疱疹病毒(KSHV)被发现后不久,人们就认识到这种病毒与大多数感染人类免疫缺陷病毒的患者中出现的多中心Castleman病(MCD)病例有关。随后人们认识到,KSHV相关的MCD是一种与其他形式的MCD不同的实体。与与KSHV无关的MCD一样,KSHV相关的MCD的临床表现以全身炎症症状为主,包括发热、恶病质,实验室异常包括血细胞减少、低白蛋白血症、低钠血症和C反应蛋白升高。病理上,KSHV相关的MCD的特征是在受影响淋巴结的滤泡内区域有多克隆、IgM-λ限制性浆细胞样细胞。这些细胞中的一部分被KSHV感染,并且这些细胞中有相当一部分表达KSHV裂解基因,包括白细胞介素-6(IL-6)的病毒同源物(vIL-6)。KSHV相关的MCD患者外周血中的KSHV病毒载量通常会升高。vIL-6的产生和人(h)IL-6的诱导都导致症状,可能与IL-10和其他细胞因子的过度产生共同作用。直到最近,KSHV相关的MCD患者的预后都很差。最近,用抗CD20单克隆抗体利妥昔单抗靶向KSHV感染的B细胞以及利用KSHV酶靶向KSHV感染细胞的治疗进展显著改善了患者的预后。最近,另一种与KSHV相关的病症,即KSHV炎性细胞因子综合征(KICS)已被描述。其临床表现类似于KSHV相关的MCD,但淋巴结病不突出,且没有KSHV相关的MCD的病理性淋巴结改变。KICS患者的KSHV病毒载量升高,vIL-6、人白细胞介素-6同源物和IL-10升高,与KSHV相关的MCD中所见的情况相当;这些物质的细胞来源尚待研究。KICS可能导致一些严重卡波西肉瘤或原发性渗出性淋巴瘤患者出现炎症症状。需要更多的研究来更好地界定KICS的临床范围及其与KSHV相关的MCD的关系。此外,需要进行研究以更好地了解KICS和KSHV相关的MCD的发病机制和流行病学,以及这两种疾病的最佳治疗方法。