Department of Congenital Heart Disease and Pediatric Cardiology, Deutsches Herzzentrum Berlin, Augustenburger Platz 1, Berlin 13353, Germany.
J Cardiovasc Magn Reson. 2012 Mar 28;14(1):22. doi: 10.1186/1532-429X-14-22.
The short inversion time inversion recovery (STIR) black-blood technique has been used to visualize myocardial edema, and thus to differentiate acute from chronic myocardial lesions. However, some cardiovascular magnetic resonance (CMR) groups have reported variable image quality, and hence the diagnostic value of STIR in routine clinical practice has been put into question. The aim of our study was to analyze image quality and diagnostic performance of STIR using a set of pulse sequence parameters dedicated to edema detection, and to discuss possible factors that influence image quality. We hypothesized that STIR imaging is an accurate and robust way of detecting myocardial edema in non-selected patients with acute myocardial infarction.
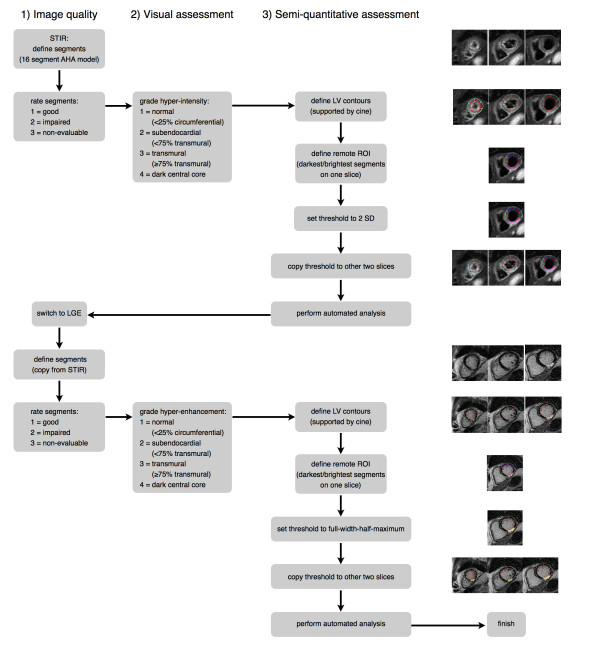
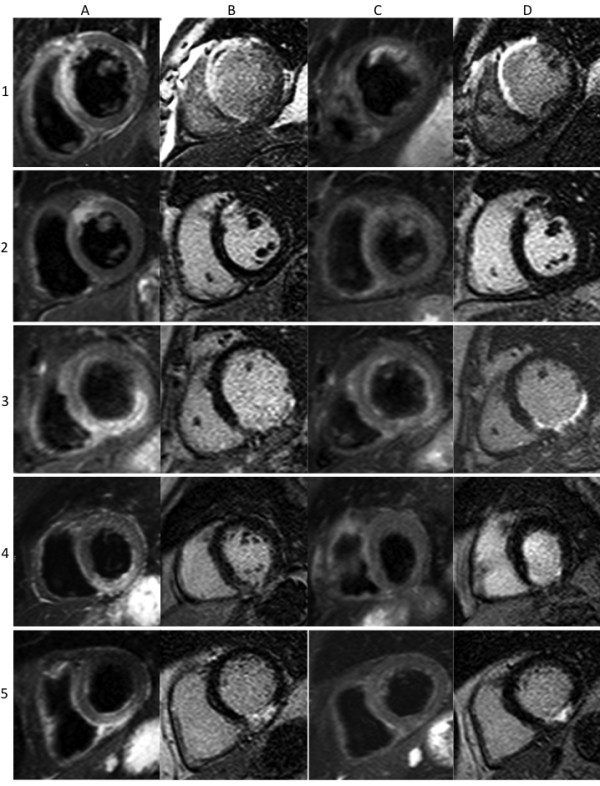
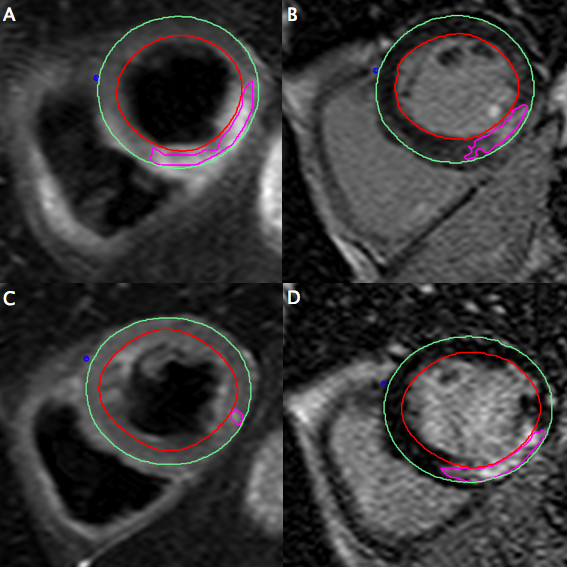
Forty-six consecutive patients with acute myocardial infarction underwent CMR (day 4.5, +/- 1.6) including STIR for the assessment of myocardial edema and late gadolinium enhancement (LGE) for quantification of myocardial necrosis. Thirty of these patients underwent a follow-up CMR at approximately six months (195 +/- 39 days). Both STIR and LGE images were evaluated separately on a segmental basis for image quality as well as for presence and extent of myocardial hyper-intensity, with both visual and semi-quantitative (threshold-based) analysis. LGE was used as a reference standard for localization and extent of myocardial necrosis (acute) or scar (chronic).
Image quality of STIR images was rated as diagnostic in 99.5% of cases. At the acute stage, the sensitivity and specificity of STIR to detect infarcted segments on visual assessment was 95% and 78% respectively, and on semi-quantitative assessment was 99% and 83%, respectively. STIR differentiated acutely from chronically infarcted segments with a sensitivity of 95% by both methods and with a specificity of 99% by visual assessment and 97% by semi-quantitative assessment. The extent of hyper-intense areas on acute STIR images was 85% larger than those on LGE images, with a larger myocardial salvage index in reperfused than in non-reperfused infarcts (p = 0.035).
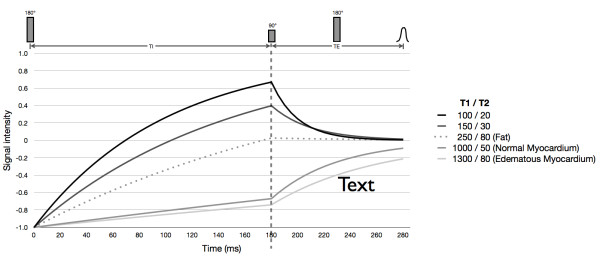
STIR with appropriate pulse sequence settings is accurate in detecting acute myocardial infarction (MI) and distinguishing acute from chronic MI with both visual and semi-quantitative analysis. Due to its unique technical characteristics, STIR should be regarded as an edema-weighted rather than a purely T2-weighted technique.
短反转时间反转恢复(STIR)黑血技术已被用于可视化心肌水肿,从而区分急性和慢性心肌病变。然而,一些心血管磁共振(CMR)组报告了可变的图像质量,因此 STIR 在常规临床实践中的诊断价值受到了质疑。我们的研究目的是分析使用专门用于水肿检测的一组脉冲序列参数的 STIR 的图像质量和诊断性能,并讨论可能影响图像质量的因素。我们假设 STIR 成像在急性心肌梗死的非选择性患者中是一种准确且可靠的检测心肌水肿的方法。
46 例连续的急性心肌梗死患者接受 CMR(第 4.5 天,+/-1.6 天)检查,包括 STIR 以评估心肌水肿和晚期钆增强(LGE)以定量评估心肌坏死。其中 30 例患者在大约 6 个月(195+/-39 天)时进行了随访 CMR。STIR 和 LGE 图像均分别进行节段性评估,评估图像质量以及心肌高信号的存在和程度,包括视觉评估和半定量(基于阈值)分析。LGE 被用作心肌坏死(急性)或瘢痕(慢性)定位和程度的参考标准。
STIR 图像的质量在 99.5%的病例中被评为诊断性。在急性期,STIR 在视觉评估上检测梗死节段的敏感性和特异性分别为 95%和 78%,在半定量评估上分别为 99%和 83%。STIR 通过两种方法分别以 95%的敏感性和 99%的特异性和 97%的半定量评估区分急性和慢性梗死节段。急性 STIR 图像上高信号区域的范围比 LGE 图像大 85%,再灌注性梗死与非再灌注性梗死的心肌挽救指数更大(p=0.035)。
使用适当的脉冲序列设置的 STIR 可准确检测急性心肌梗死(MI),并通过视觉和半定量分析区分急性和慢性 MI。由于其独特的技术特点,STIR 应被视为一种水肿加权而非纯 T2 加权技术。