Morell Emily, Wolfe Joanne, Scheurer Mark, Thiagarajan Ravi, Morin Caroline, Beke Dorothy M, Smoot Leslie, Cheng Henry, Gauvreau Kimberlee, Blume Elizabeth D
Harvard Medical School, Boston, Massachusetts, USA.
Arch Pediatr Adolesc Med. 2012 Aug;166(8):745-8. doi: 10.1001/archpediatrics.2011.1829.
To describe patterns of care for pediatric patients with advanced heart disease who experience in-hospital death.
Retrospective single-institution medical record review.
A tertiary care pediatric hospital.
All patients younger than 21 years who died in the inpatient setting between January 1, 2007, and December 31, 2009, with primary cardiac diagnoses or who had ever received a cardiology consult (N=468). After excluding patients with significant noncardiac primary diagnoses, 111 children formed the analytic sample.
In-hospital deaths of children with heart disease during a 3-year period.
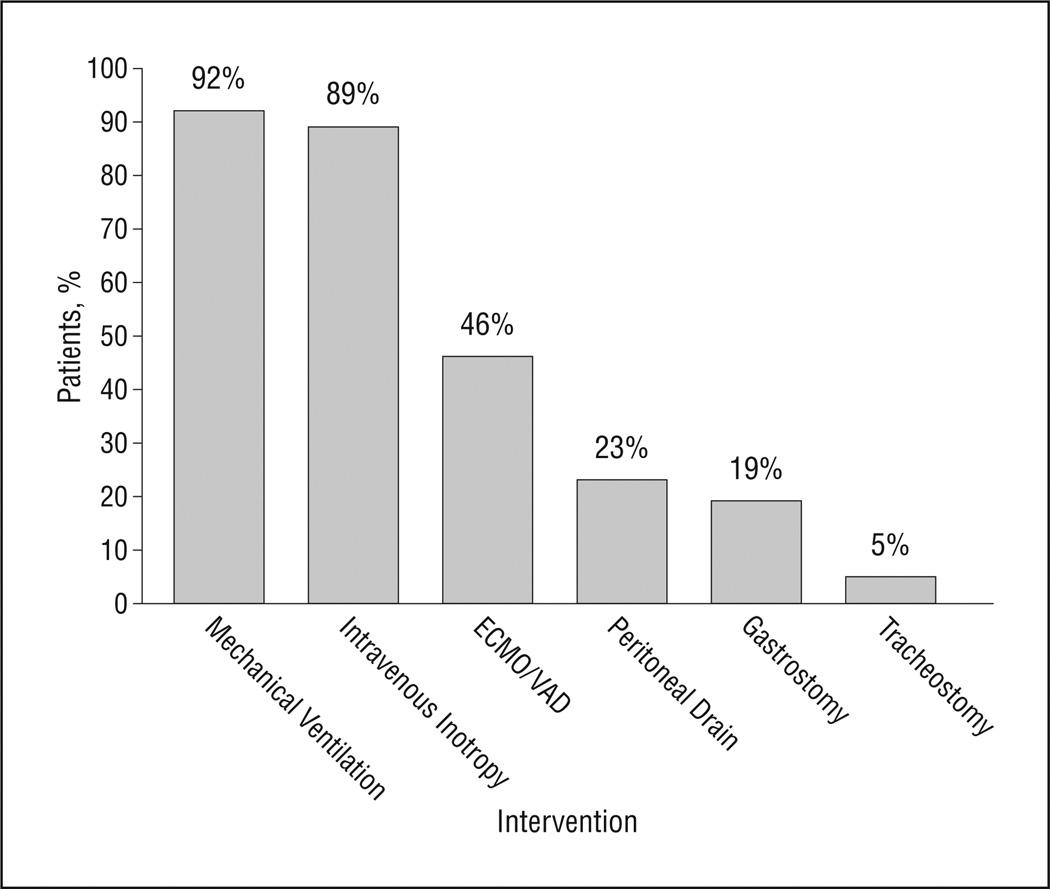
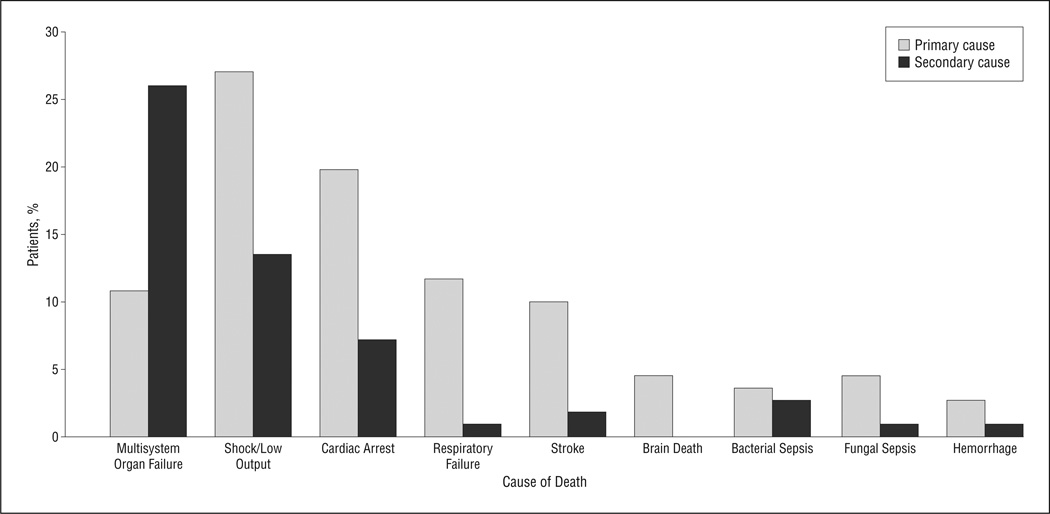
Median age at death was 4.8 months (age range,1 day to 20.5 years), with 84 deaths (75.7%) occurring before age 1 year. Median length of terminal hospital stay was 22 days (range, 1-199 days). Diagnoses included 84 patients (75.7%) with congenital heart disease, 10 (9.0%)with cardiomyopathy/myocarditis, 9 (8.1%) with pulmonary hypertension, and 8 (7.2%) with heart transplants.Sixty-two patients (55.9%) had received cardio-pulmonary resuscitation during their last hospital admission. At the end of life, 21 children (18.9%) had gastrostomy tubes and 26 (23.4%) had peritoneal drains.Most patients (91.9%) received ventilation, with half also receiving mechanical circulatory support. Eighty-three patients (74.8%) experienced additional end-organ failure. Classified by mode of death, 76 patients (68.5%) had disease-directed support withdrawn, 28 (25.2%) died during resuscitation, and 7 (6.3%) died while receiving comfort care after birth. Eighty-three percent of parents were present at the time of death.
Infants and children who die of advanced heart disease frequently succumb in the intensive care setting with multisystem organ failure and exposure to highly technical care.
描述患有晚期心脏病的儿科患者在医院死亡的护理模式。
回顾性单机构病历审查。
一家三级护理儿科医院。
2007年1月1日至2009年12月31日期间在住院环境中死亡的所有21岁以下患者,有原发性心脏诊断或曾接受过心脏病咨询(N = 468)。排除有重大非心脏原发性诊断的患者后,111名儿童构成分析样本。
3年期间患有心脏病儿童的院内死亡情况。
死亡时的中位年龄为4.8个月(年龄范围为1天至20.5岁),84例死亡(75.7%)发生在1岁之前。终末期住院时间的中位数为22天(范围为1 - 199天)。诊断包括84例(75.7%)先天性心脏病患者、10例(9.0%)心肌病/心肌炎患者、9例(8.1%)肺动脉高压患者和8例(7.2%)心脏移植患者。62例患者(55.9%)在最后一次住院期间接受了心肺复苏。临终时,21名儿童(18.9%)有胃造瘘管,26名(23.4%)有腹腔引流管。大多数患者(91.9%)接受了通气,其中一半还接受了机械循环支持。83例患者(74.8%)出现了额外的终末器官衰竭。按死亡方式分类,76例患者(68.5%)停止了针对疾病的支持治疗,28例(25.2%)在复苏过程中死亡,7例(6.3%)在出生后接受舒适护理时死亡。83%的父母在孩子死亡时在场。
死于晚期心脏病的婴幼儿常在重症监护环境中因多系统器官衰竭并接受高技术护理而死亡。