Department of Cancer Prevention and Control, Roswell Park Cancer Institute, Buffalo, New York, United States of America.
PLoS One. 2012;7(3):e30950. doi: 10.1371/journal.pone.0030950. Epub 2012 Mar 27.
Family history and African-American race are important risk factors for both prostate cancer (CaP) incidence and aggressiveness. When studying complex diseases such as CaP that have a heritable component, chances of finding true disease susceptibility alleles can be increased by accounting for genetic ancestry within the population investigated. Race, ethnicity and ancestry were studied in a geographically diverse cohort of men with newly diagnosed CaP.
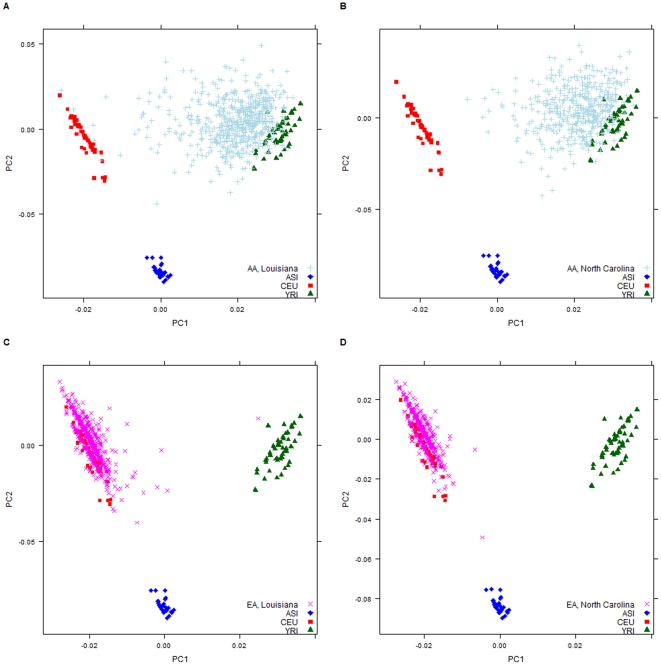
Individual ancestry (IA) was estimated in the population-based North Carolina and Louisiana Prostate Cancer Project (PCaP), a cohort of 2,106 incident CaP cases (2063 with complete ethnicity information) comprising roughly equal numbers of research subjects reporting as Black/African American (AA) or European American/Caucasian/Caucasian American/White (EA) from North Carolina or Louisiana. Mean genome wide individual ancestry estimates of percent African, European and Asian were obtained and tested for differences by state and ethnicity (Cajun and/or Creole and Hispanic/Latino) using multivariate analysis of variance models. Principal components (PC) were compared to assess differences in genetic composition by self-reported race and ethnicity between and within states.
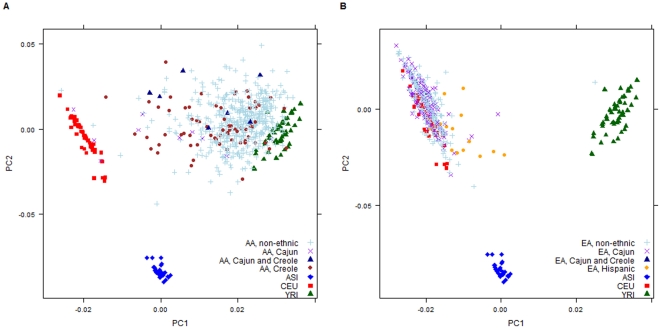
Mean individual ancestries differed by state for self-reporting AA (p = 0.03) and EA (p = 0.001). This geographic difference attenuated for AAs who answered "no" to all ethnicity membership questions (non-ethnic research subjects; p = 0.78) but not EA research subjects, p = 0.002. Mean ancestry estimates of self-identified AA Louisiana research subjects for each ethnic group; Cajun only, Creole only and both Cajun and Creole differed significantly from self-identified non-ethnic AA Louisiana research subjects. These ethnicity differences were not seen in those who self-identified as EA.
Mean IA differed by race between states, elucidating a potential contributing factor to these differences in AA research participants: self-reported ethnicity. Accurately accounting for genetic admixture in this cohort is essential for future analyses of the genetic and environmental contributions to CaP.
家族史和非裔美国人的种族是非裔美国人前列腺癌(CaP)发病率和侵袭性的重要危险因素。当研究前列腺癌等具有遗传成分的复杂疾病时,通过在研究人群中考虑遗传祖先,就有可能增加发现真正的疾病易感等位基因的机会。在一个地理上多样化的新诊断为 CaP 的男性队列中研究了种族、民族和祖先。
在基于人群的北卡罗来纳州和路易斯安那州前列腺癌项目(PCaP)中估计了个体祖先(IA),该队列包括 2106 例新诊断的 CaP 病例(2063 例具有完整种族信息),其中来自北卡罗来纳州或路易斯安那州的研究对象大致相等,报告为黑/非裔美国人(AA)或欧裔美国人/高加索人/高加索裔美国人/白人(EA)。获得了平均全基因组个体祖先估计的非洲、欧洲和亚洲百分比,并使用多元方差分析模型按州和种族(卡津人和/或克里奥尔人和西班牙裔/拉丁裔)进行了差异检验。比较了主成分(PC),以评估报告种族和族裔之间以及各州内遗传成分的差异。
报告的 AA(p = 0.03)和 EA(p = 0.001)的个体祖先因州而异。这种地理差异在对所有种族成员问题回答“否”的非裔 AA 研究对象中减弱(非种族研究对象;p = 0.78),但在 EA 研究对象中没有减弱,p = 0.002。自我认同的 AA 路易斯安那州研究对象的每个种族群体的平均祖先估计值;仅卡津人、仅克里奥尔人和卡津人和克里奥尔人都与自我认同的非裔 AA 路易斯安那州研究对象有显著差异。这些族裔差异在自我认同为 EA 的人群中并未出现。
各州之间的平均 IA 因种族而异,这说明了 AA 研究参与者之间这些差异的一个潜在促成因素:自我报告的种族。在该队列中准确地考虑遗传混合对于未来分析前列腺癌的遗传和环境贡献至关重要。