Health Services Research and Development (152), Michael E. DeBakey Veterans Affairs Medical Center, 2002 Holcombe Boulevard, Houston, TX 77030, USA.
Ann Intern Med. 2012 May 15;156(10):728-35. doi: 10.7326/0003-4819-156-10-201205150-00011.
The Department of Health and Human Services recently called for public comment on human subjects research protections.
To assess variability in reviews across institutional review boards (IRBs) for a multisite, minimal-risk trial of financial incentives for evidence-based hypertension care and to quantify the effect of review determinations on site participation, budget, and timeline.
A natural experiment occurring from multiple IRBs reviewing the same protocol for a multicenter trial (May 2005 to October 2007).
25 Veterans Affairs (VA) medical centers.
Number of submissions, time to approval, and costs were evaluated; patient complexity, academic affiliation, size, and location (urban or rural) between participating and nonparticipating VA medical centers were compared.
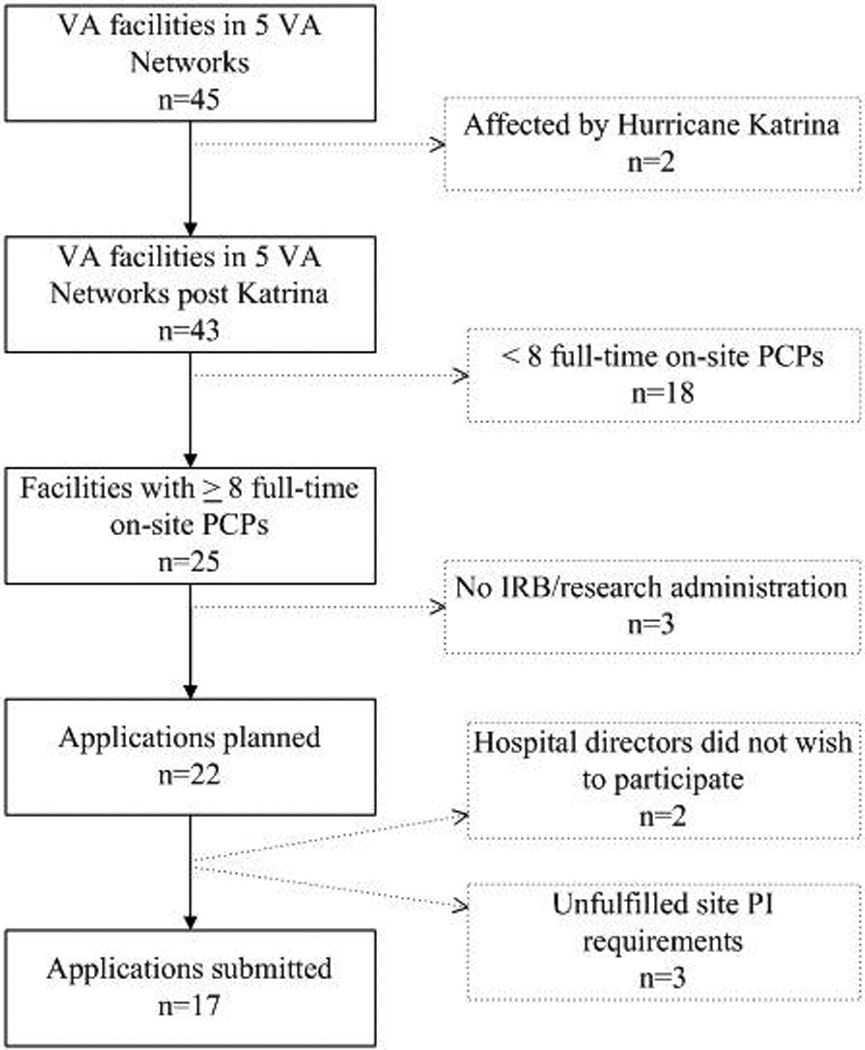
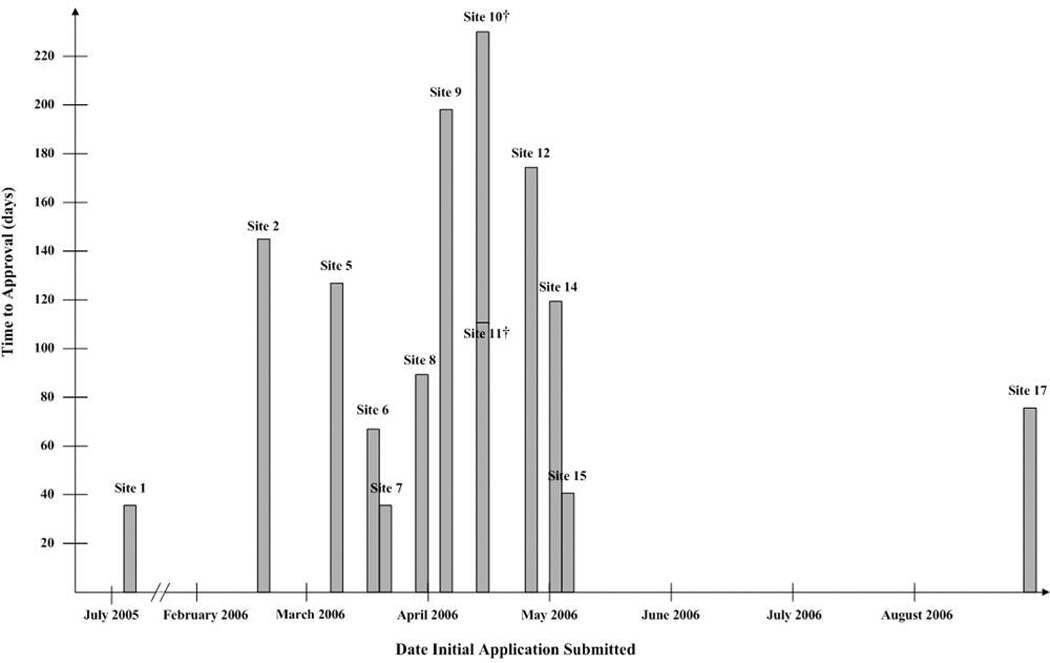
Of 25 eligible VA medical centers, 6 did not meet requirements for IRB review and 2 declined to participate. Of 17 applications, 14 were approved. The process required 115 submissions, lasted 27 months, and cost close to $170 000 in staff salaries. One IRB's concern about incentivizing a particular medication recommended by national guidelines prompted a change in our design to broaden our inclusion criteria beyond uncomplicated hypertension. The change required amending the protocol at 14 sites to preserve internal validity. The IRBs that approved the protocol classified it as minimal risk. The 12 sites that ultimately participated in the trial were more likely to be urban and academically affiliated and to care for more complex patients, which limits the external validity of the trial's findings.
Because data came from a single multisite trial in the VA system that uses a 2-stage review process, generalizability is limited.
Complying with IRB requirements for a minimal-risk study required substantial resources and threatened the study's internal and external validity. The current review of regulatory requirements may address some of these problems.
美国卫生与公众服务部最近就人体研究保护措施征求公众意见。
评估多个机构审查委员会(IRB)对一项基于财务激励的证据为基础的高血压护理的多地点、低风险试验的审查变异性,并量化审查决定对参与、预算和时间表的影响。
一项自然实验,涉及多个 IRB 审查同一协议的多中心试验(2005 年 5 月至 2007 年 10 月)。
25 个退伍军人事务部(VA)医疗中心。
评估提交的数量、批准时间和成本;比较参与和不参与 VA 医疗中心的患者复杂性、学术隶属关系、大小和位置(城市或农村)。
在 25 个符合条件的 VA 医疗中心中,有 6 个不符合 IRB 审查要求,有 2 个拒绝参与。在 17 项申请中,有 14 项获得批准。该过程需要 115 次提交,历时 27 个月,员工工资接近 17 万美元。一个 IRB 对激励国家指南推荐的特定药物的担忧促使我们改变设计,将纳入标准扩大到不仅仅是简单的高血压。这一变化要求在 14 个地点修改方案,以保持内部有效性。批准方案的 IRB 将其归类为低风险。最终参与试验的 12 个地点更有可能是城市和学术附属机构,并且治疗更复杂的患者,这限制了试验结果的外部有效性。
由于数据来自退伍军人事务部系统中的一项单一的多地点试验,使用了两阶段审查过程,因此推广性有限。
遵守 IRB 对低风险研究的要求需要大量资源,并威胁到研究的内部和外部有效性。目前对监管要求的审查可能会解决其中的一些问题。