Division of Basic Biomedical Sciences, Sanford School of Medicine of The University of South Dakota, 414 East Clark Street, Vermillion, SD, USA.
BMC Cancer. 2012 Jun 22;12:200. doi: 10.1186/1471-2407-12-200.
Advanced ovarian cancer is treated with cytoreductive surgery and combination platinum- and taxane-based chemotherapy. Although most patients have acute clinical response to this strategy, the disease ultimately recurs. In this work we questioned whether the synthetic steroid mifepristone, which as monotherapy inhibits the growth of ovarian cancer cells, is capable of preventing repopulation of ovarian cancer cells if given after a round of lethal cisplatin-paclitaxel combination treatment.
We established an in vitro approach wherein ovarian cancer cells with various sensitivities to cisplatin or paclitaxel were exposed to a round of lethal doses of cisplatin for 1 h plus paclitaxel for 3 h. Thereafter, cells were maintained in media with or without mifepristone, and short- and long-term cytotoxicity was assessed.
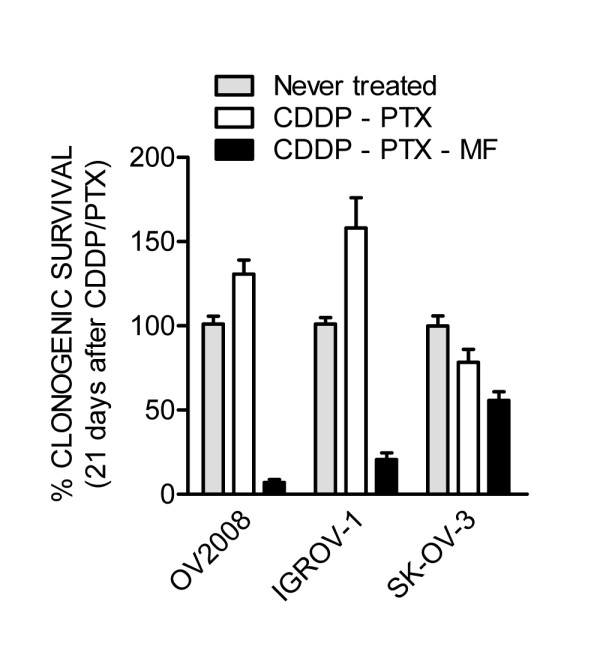
Four days after treatment the lethality of cisplatin-paclitaxel was evidenced by reduced number of cells, increased hypodiploid DNA content, morphological features of apoptosis, DNA fragmentation, and cleavage of caspase-3, and of its downstream substrate PARP. Short-term presence of mifepristone either enhanced or did not modify such acute lethality. Seven days after receiving cisplatin-paclitaxel, cultures showed signs of relapse with escaping colonies that repopulated the plate in a time-dependent manner. Conversely, cultures exposed to cisplatin-paclitaxel followed by mifepristone not only did not display signs of repopulation following initial chemotherapy, but they also had their clonogenic capacity drastically reduced when compared to cells repopulating after cisplatin-paclitaxel.
Cytostatic concentrations of mifepristone after exposure to lethal doses of cisplatin and paclitaxel in combination blocks repopulation of remnant cells surviving and escaping the cytotoxic drugs.
高级卵巢癌采用细胞减灭术和联合铂类和紫杉烷类化疗治疗。尽管大多数患者对这种策略有急性临床反应,但疾病最终仍会复发。在这项工作中,我们质疑是否合成类固醇米非司酮,作为单一疗法抑制卵巢癌细胞的生长,如果在一轮致死性顺铂-紫杉醇联合治疗后给予,是否能够阻止卵巢癌细胞的再增殖。
我们建立了一种体外方法,其中对各种顺铂或紫杉醇敏感性的卵巢癌细胞暴露于 1 小时顺铂加 3 小时紫杉醇的一轮致死剂量下。此后,将细胞维持在含有或不含有米非司酮的培养基中,并评估短期和长期细胞毒性。
治疗后 4 天,顺铂-紫杉醇的致死性通过减少细胞数量、增加低倍体 DNA 含量、凋亡的形态特征、DNA 片段化和 caspase-3 及其下游底物 PARP 的裂解来证明。米非司酮的短期存在增强或不改变这种急性致死性。接受顺铂-紫杉醇治疗 7 天后,培养物显示出复发的迹象,逃避的集落以时间依赖性方式重新填充平板。相反,暴露于顺铂-紫杉醇后再暴露于米非司酮的培养物不仅在初始化疗后没有显示再增殖的迹象,而且与顺铂-紫杉醇后再增殖的细胞相比,其集落形成能力大大降低。
在联合使用致死剂量的顺铂和紫杉醇后,米非司酮的细胞抑制浓度可阻止存活和逃避细胞毒药物的残余细胞再增殖。