School of Population Health, University of Queensland, Herston 4029, Australia.
BMC Public Health. 2012 Jun 1;12:398. doi: 10.1186/1471-2458-12-398.
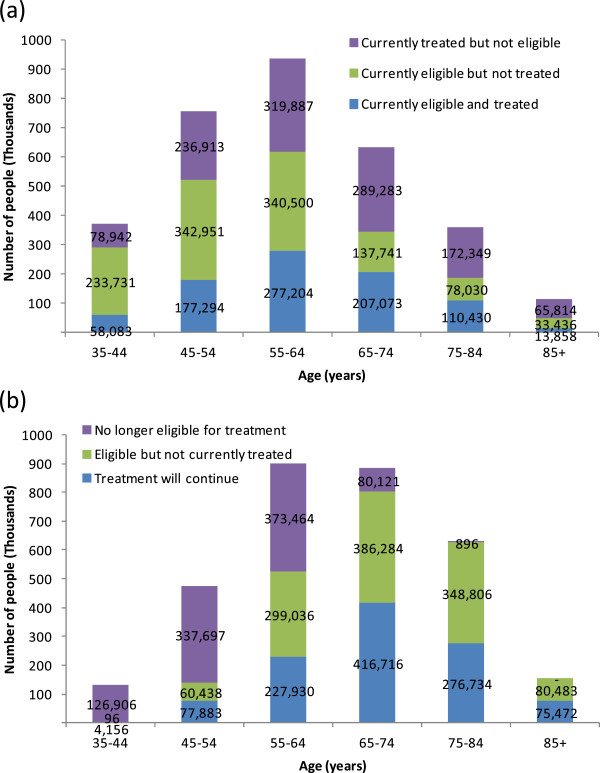
Cardiovascular disease is the leading cause of death worldwide. Like many countries, Australia is currently changing its guidelines for cardiovascular disease prevention from drug treatment for everyone with 'high blood pressure' or 'high cholesterol', to prevention based on a patient's absolute risk. In this research, we model cost-effectiveness of cardiovascular disease prevention with blood pressure and lipid drugs in Australia under three different scenarios: (1) the true current practice in Australia; (2) prevention as intended under the current guidelines; and (3) prevention according to proposed absolute risk levels. We consider the implications of changing to absolute risk-based cardiovascular disease prevention, for the health of the Australian people and for Government health sector expenditure over the long term.
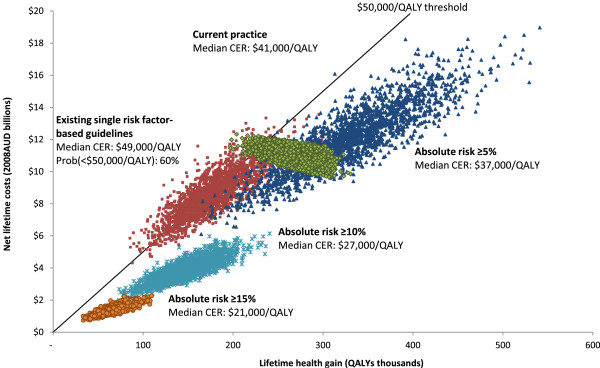
We evaluate cost-effectiveness of statins, diuretics, ACE inhibitors, calcium channel blockers and beta-blockers, for Australian men and women, aged 35 to 84 years, who have never experienced a heart disease or stroke event. Epidemiological changes and health care costs are simulated by age and sex in a discrete time Markov model, to determine total impacts on population health and health sector costs over the lifetime, from which we derive cost-effectiveness ratios in 2008 Australian dollars per quality-adjusted life year.
Cardiovascular disease prevention based on absolute risk is more cost-effective than prevention under the current guidelines based on single risk factor thresholds, and is more cost-effective than the current practice, which does not follow current clinical guidelines. Recommending blood pressure-lowering drugs to everyone with at least 5% absolute risk and statin drugs to everyone with at least 10% absolute risk, can achieve current levels of population health, while saving $5.4 billion for the Australian Government over the lifetime of the population. But savings could be as high as $7.1 billion if Australia could match the cheaper price of statin drugs in New Zealand.
Changing to absolute risk-based cardiovascular disease prevention is highly recommended for reducing health sector spending, but the Australian Government must also consider measures to reduce the cost of statin drugs, over and above the legislated price cuts of November 2010.
心血管疾病是全球范围内的主要致死原因。与许多国家一样,澳大利亚目前正在改变其心血管疾病预防指南,从对所有“高血压”或“高胆固醇”患者进行药物治疗,转变为基于患者绝对风险的预防措施。在这项研究中,我们针对澳大利亚的血压和血脂药物在三种不同情况下的心血管疾病预防的成本效益进行建模:(1)澳大利亚当前的真实实践;(2)现行指南中预期的预防;(3)根据建议的绝对风险水平进行预防。我们考虑了转向基于绝对风险的心血管疾病预防对澳大利亚人民健康和政府卫生部门长期支出的影响。
我们评估了他汀类药物、利尿剂、血管紧张素转换酶抑制剂、钙通道阻滞剂和β受体阻滞剂在从未经历过心脏病或中风的 35 至 84 岁澳大利亚男性和女性中的成本效益。通过年龄和性别在离散时间马尔可夫模型中模拟流行病学变化和医疗保健成本,以确定对人口健康和卫生部门成本的终生总影响,从而根据 2008 年澳大利亚元计算每质量调整生命年的成本效益比。
基于绝对风险的心血管疾病预防比基于单一风险因素阈值的现行指南更具成本效益,也比不遵循现行临床指南的现行做法更具成本效益。建议至少有 5%绝对风险的人使用降压药物,至少有 10%绝对风险的人使用他汀类药物,可以达到当前的人口健康水平,同时为澳大利亚政府节省 54 亿美元的终生支出。但如果澳大利亚能够效仿新西兰降低他汀类药物的价格,节省额可能高达 71 亿美元。
强烈建议转向基于绝对风险的心血管疾病预防,以减少卫生部门的支出,但澳大利亚政府还必须考虑采取措施降低他汀类药物的成本,以弥补 2010 年 11 月立法降价之外的成本。