Department of General Practice and the EMGO + Institute for Health and Care Research (EMGO+), VU University medical Centre, Amsterdam, The Netherlands.
BMC Psychiatry. 2012 Jun 7;12:59. doi: 10.1186/1471-244X-12-59.
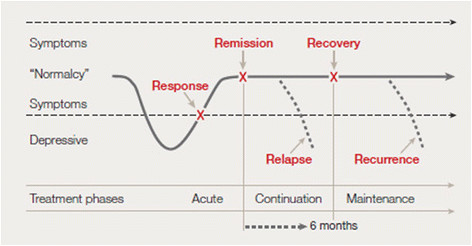
Major Depressive Disorder is a leading cause of disability, tends to run a recurrent course and is associated with substantial economic costs due to increased healthcare utilization and productivity losses. Interventions aimed at the prevention of recurrences may reduce patients' suffering and costs. Besides antidepressants, several psychological treatments such as preventive cognitive therapy (PCT) are effective in the prevention of recurrences of depression. Yet, many patients find long-term use of antidepressants unattractive, do not want to engage in therapy sessions and in the primary care setting psychologists are often not available. Therefore, it is important to study whether PCT can be used in a nurse-led self-help format in primary care. This study sets out to test the hypothesis that usual care plus nurse-led self-help for recurrent depression in primary care is feasible, acceptable and cost-effective compared to usual care only.
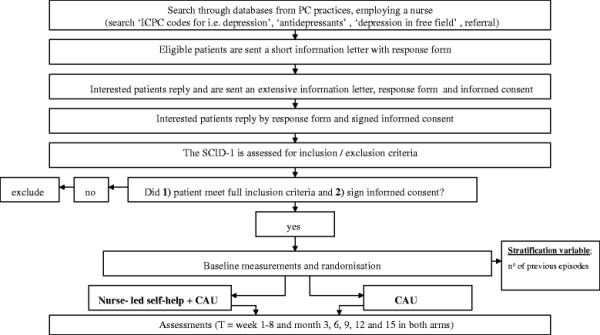
Patients are randomly assigned to 'nurse-led self-help treatment plus usual care' (134 participants) or 'usual care' (134 participants). Randomisation is stratified according to the number of previous episodes (2 or 3 previous episodes versus 4 or more). The primary clinical outcome is the cumulative recurrence rate of depression meeting DSM-IV criteria as assessed by the Structured-Clinical-Interview-for-DSM-IV- disorders at one year after completion of the intervention. Secondary clinical outcomes are quality of life, severity of depressive symptoms, co-morbid psychopathology and self-efficacy. As putative effect-moderators, demographic characteristics, number of previous episodes, type of treatment during previous episodes, age of onset, self-efficacy and symptoms of pain and fatigue are assessed. Cumulative recurrence rate ratios are obtained under a Poisson regression model. Number-needed-to-be-treated is calculated as the inverse of the risk-difference. The economic evaluation is conducted from a societal perspective, both as a cost-effectiveness analysis (costs per depression free survival year) and as a cost-utility analysis (costs per quality adjusted life-year).
The purpose of this paper is to outline the rationale and design of a nurse-led, cognitive therapy based self-help aimed at preventing recurrence of depression in a primary care setting. Only few studies have focused on psychological self-help interventions aimed at the prevention of recurrences in primary care patients.
NTR3001 (http://www.trialregister.nl).
重度抑郁症是导致残疾的主要原因之一,往往反复发作,并且由于医疗保健利用增加和生产力损失而导致大量经济成本。旨在预防复发的干预措施可能会减轻患者的痛苦和成本。除抗抑郁药外,预防认知疗法(PCT)等几种心理疗法在预防抑郁症复发方面也很有效。然而,许多患者发现长期使用抗抑郁药不可取,不想接受治疗,而且在初级保健环境中,心理学家通常也无法提供帮助。因此,研究 PCT 是否可以在初级保健中以护士主导的自助形式使用非常重要。本研究旨在检验以下假设:与仅常规护理相比,常规护理加护士主导的反复发作性抑郁症自助治疗在初级保健中是可行、可接受且具有成本效益的。
患者被随机分配到“护士主导的自助治疗加常规护理”(134 名参与者)或“常规护理”(134 名参与者)。随机分组根据之前发作的次数进行分层(2 或 3 次发作与 4 次或更多次发作)。主要临床结局是在干预完成一年后,通过 DSM-IV 障碍的结构化临床访谈-IV 评估符合 DSM-IV 标准的抑郁复发累积发生率。次要临床结局是生活质量、抑郁症状严重程度、合并精神病理学和自我效能感。作为可能的效应调节剂,评估人口统计学特征、之前发作的次数、之前发作期间的治疗类型、发病年龄、自我效能感以及疼痛和疲劳症状。使用泊松回归模型获得累积复发率比。计算需要治疗的人数作为风险差异的倒数。经济评估从社会角度进行,既进行成本效益分析(无抑郁生存年的成本效益分析),又进行成本效用分析(质量调整生命年的成本效益分析)。
本文旨在概述一种基于认知疗法的护士主导的自助治疗方案,该方案旨在预防初级保健患者的抑郁复发。只有少数研究侧重于旨在预防初级保健患者复发的心理自助干预措施。
NTR3001(http://www.trialregister.nl)。