King's College London British Heart Foundation Centre of Excellence, London, United Kingdom.
J Cardiovasc Magn Reson. 2012 Jun 9;14(1):34. doi: 10.1186/1532-429X-14-34.
Technical advances in perfusion cardiovascular magnetic resonance (CMR), particularly accelerated data acquisition methods, allow myocardial perfusion imaging with unprecedented spatial resolution. However, it is not clear how implementation of these recent advances affects perfusion image quality, signal and contrast to noise ratios (SNR & CNR) and the occurrence of important artefacts in routine clinical imaging. The objective of this study was therefore to compare a standard and an advanced, high-resolution perfusion sequence.
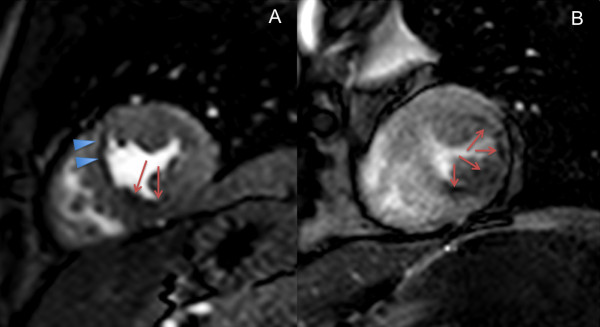
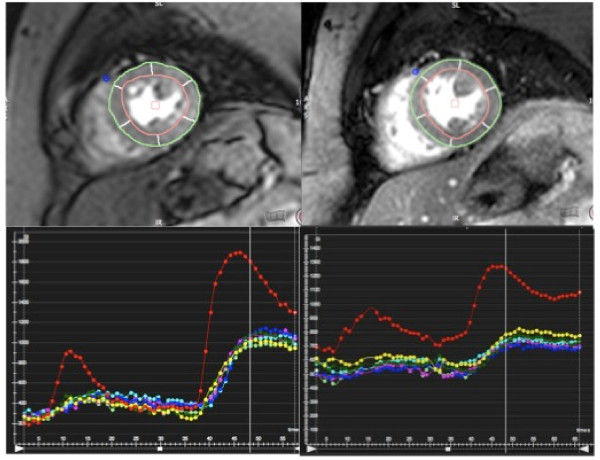
A standard ultrafast gradient echo perfusion sequence (st-GrE) was compared with an advanced kt-accelerated steady state free precession sequence (ktBLAST-SSFP) at 1.5 T in healthy volunteers (n = 16) and in patients (n = 32) with known or suspected coronary artery disease. Volunteers were imaged with both sequences at rest and patients underwent stress and rest imaging with either st-GrE or ktBLAST-SSFP prior to X-ray coronary angiography.A blinded expert scored image quality and respiratory artefact severity and also classified patients for the presence of CAD. The extent, transmurality and duration of dark rim artefacts (DRA) as well as signal to noise (SNR) and contrast to noise (CNR) were quantified.
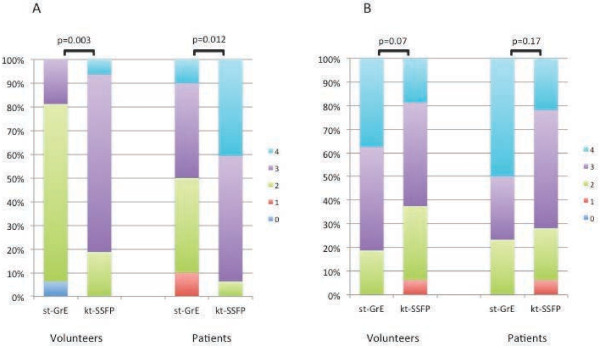
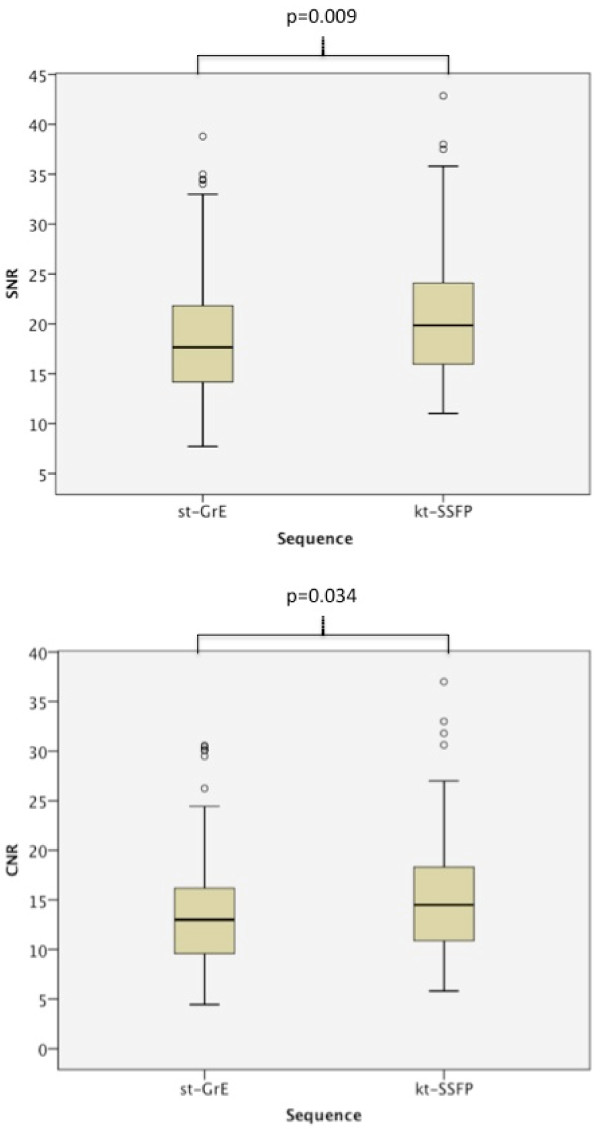
In normal hearts ktBLAST-SSFP imaging resulted in significantly improved image quality (p = 0.003), SNR (21.0 ± 6.7 vs. 18.8 ± 6.6; p = 0.009), CNR (15.4 ± 6.1 vs. 14.0 ± 6.0; p = 0.034) and a reduced extent (p = <0.0001) and transmurality (p = 0.0001) of DRA. In patients ktBLAST-SSFP imaging resulted in significantly improved image quality (p = 0.012), and a reduced extent (p = <0.0001), duration (p = 0.004) and transmurality (p = <0.0001) of DRA. Sensitivity and specificity for the detection of CAD against X-ray angiography was comparable with both sequences. There was a non-significant trend towards increased respiratory artefacts with ktBLAST-SSFP in both patients and volunteers.
Advanced high resolution perfusion CMR using a k-t-accelerated SSFP technique results in significantly improved image quality, SNR and CNR and a reduction in the extent and transmurality of DRA compared to a standard sequence. These findings support the use of advanced perfusion sequences for clinical perfusion imaging however further studies exploring whether this results in improved diagnostic accuracy are required.
灌注心血管磁共振(CMR)技术的进步,特别是加速数据采集方法,使得心肌灌注成像具有前所未有的空间分辨率。然而,目前尚不清楚这些新技术的应用如何影响灌注图像质量、信号与噪声比(SNR 和 CNR)以及在常规临床成像中重要伪影的发生。本研究的目的是比较标准和先进的高分辨率灌注序列。
在健康志愿者(n=16)和已知或疑似冠心病患者(n=32)中,我们在 1.5T 下比较了标准的超快梯度回波灌注序列(st-GrE)和先进的 kt 加速稳态自由进动序列(ktBLAST-SSFP)。志愿者在静息状态下接受两种序列的成像,患者在进行静息和应激成像前,接受 st-GrE 或 ktBLAST-SSFP 检查,然后进行 X 射线冠状动脉造影。一位盲法专家对图像质量和呼吸伪影严重程度进行评分,并对 CAD 患者进行分类。还定量评估了暗边伪影(DRA)的范围、透壁性和持续时间,以及信号与噪声(SNR)和对比与噪声(CNR)。
在正常心脏中,ktBLAST-SSFP 成像可显著提高图像质量(p=0.003)、SNR(21.0±6.7 比 18.8±6.6;p=0.009)、CNR(15.4±6.1 比 14.0±6.0;p=0.034),并减少 DRA 的范围(p<0.0001)和透壁性(p=0.0001)。在患者中,ktBLAST-SSFP 成像可显著提高图像质量(p=0.012),并减少 DRA 的范围(p<0.0001)、持续时间(p=0.004)和透壁性(p<0.0001)。与 X 射线血管造影相比,两种序列检测 CAD 的敏感性和特异性相当。在患者和志愿者中,ktBLAST-SSFP 成像的呼吸伪影呈非显著增加趋势。
与标准序列相比,使用 k-t 加速 SSFP 技术的先进高分辨率灌注 CMR 可显著提高图像质量、SNR 和 CNR,并减少 DRA 的范围和透壁性。这些发现支持使用先进的灌注序列进行临床灌注成像,但需要进一步研究以确定其是否能提高诊断准确性。