Division of Imaging Sciences, The Rayne Institute, London, UK.
J Cardiovasc Magn Reson. 2011 May 24;13(1):28. doi: 10.1186/1532-429X-13-28.
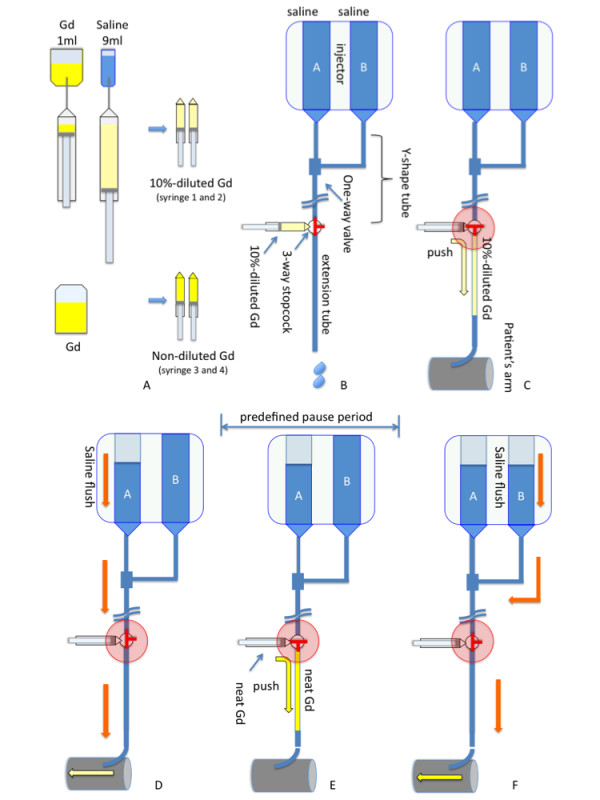
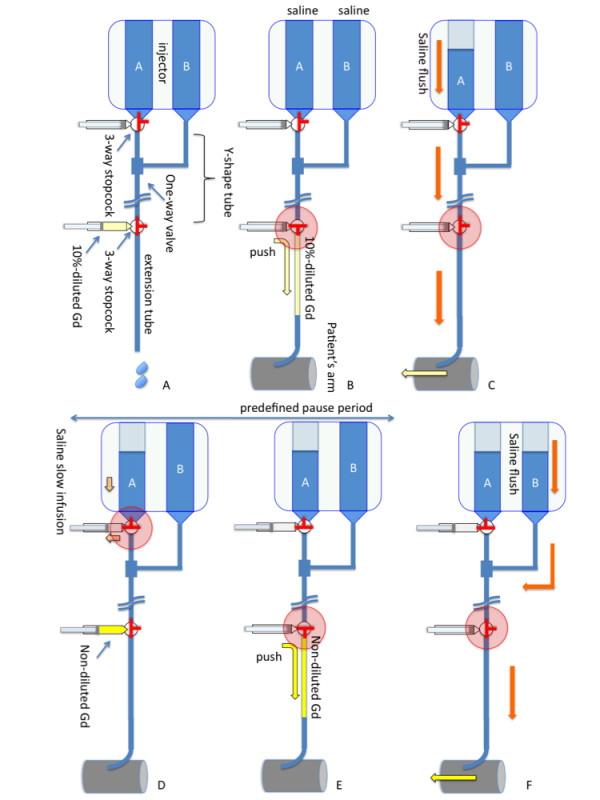
The dual-bolus protocol enables accurate quantification of myocardial blood flow (MBF) by first-pass perfusion cardiovascular magnetic resonance (CMR). However, despite the advantages and increasing demand for the dual-bolus method for accurate quantification of MBF, thus far, it has not been widely used in the field of quantitative perfusion CMR. The main reasons for this are that the setup for the dual-bolus method is complex and requires a state-of-the-art injector and there is also a lack of post processing software. As a solution to one of these problems, we have devised a universal dual-bolus injection scheme for use in a clinical setting. The purpose of this study is to show the setup and feasibility of the universal dual-bolus injection scheme.
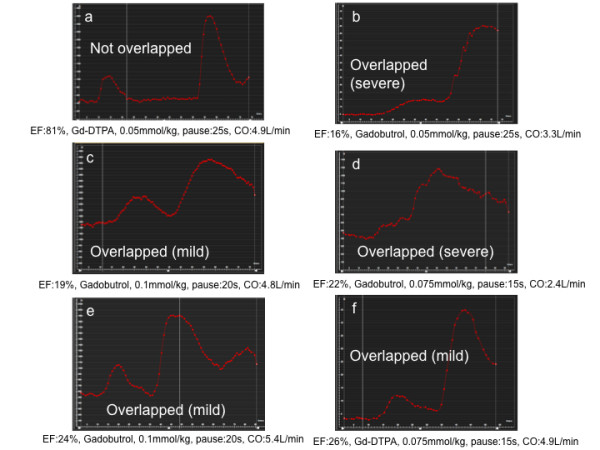
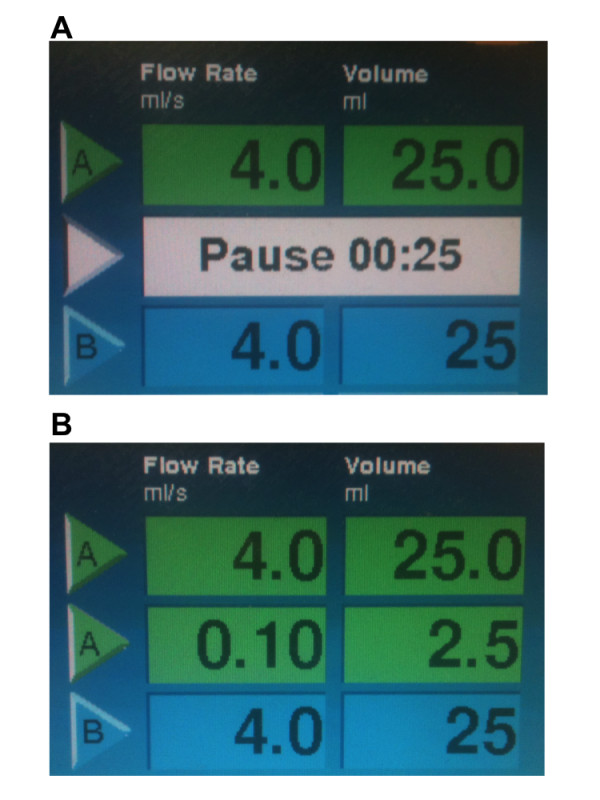
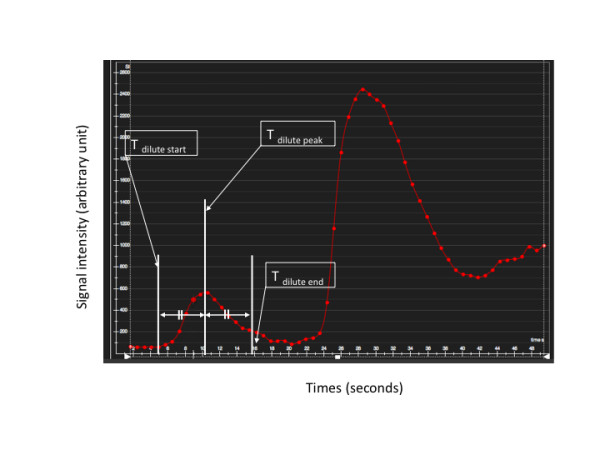
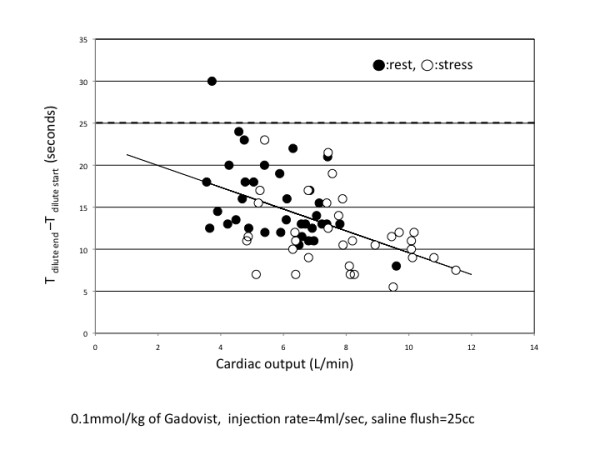
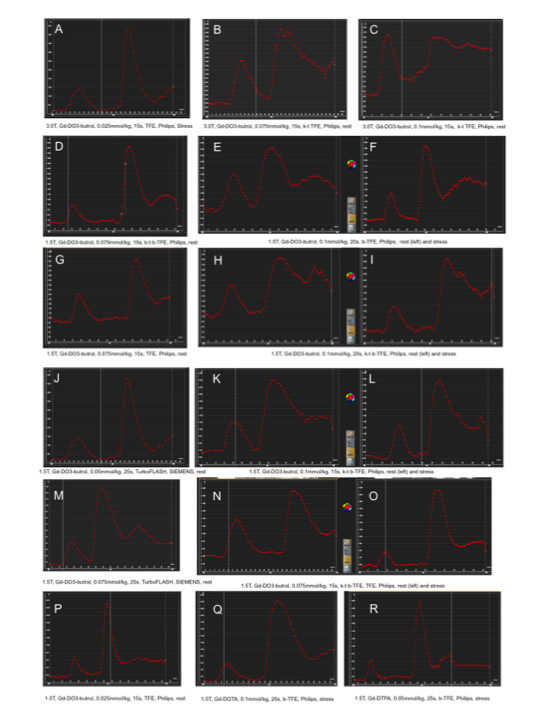
The universal dual-bolus injection scheme was tested using multiple combinations of different contrast agents, contrast agent dose, power injectors, perfusion sequences, and CMR scanners. This included 3 different contrast agents (Gd-DO3A-butrol, Gd-DTPA and Gd-DOTA), 4 different doses (0.025 mmol/kg, 0.05 mmol/kg, 0.075 mmol/kg and 0.1 mmol/kg), 2 different types of injectors (with and without "pause" function), 5 different sequences (turbo field echo (TFE), balanced TFE, k-space and time (k-t) accelerated TFE, k-t accelerated balanced TFE, turbo fast low-angle shot) and 3 different CMR scanners from 2 different manufacturers. The relation between the time width of dilute contrast agent bolus curve and cardiac output was obtained to determine the optimal predefined pause duration between dilute and neat contrast agent injection.
161 dual-bolus perfusion scans were performed. Three non-injector-related technical errors were observed (1.9%). No injector-related errors were observed. The dual-bolus scheme worked well in all the combinations of parameters if the optimal predefined pause was used. Linear regression analysis showed that the optimal duration for the predefined pause is 25s to separate the dilute and neat contrast agent bolus curves if 0.1 mmol/kg dose of Gd-DO3A-butrol is used.
The universal dual-bolus injection scheme does not require sophisticated double-head power injector function and is a feasible technique to obtain reasonable arterial input function curves for absolute MBF quantification.
通过首过灌注心血管磁共振(CMR),双脉冲方案可实现心肌血流(MBF)的精确定量。然而,尽管双脉冲方法在准确量化 MBF 方面具有优势且需求日益增加,但迄今为止,它尚未在定量灌注 CMR 领域得到广泛应用。造成这种情况的主要原因是双脉冲方法的设置复杂,需要先进的注射器,并且还缺乏后处理软件。作为解决其中一个问题的方法,我们设计了一种通用的双脉冲注射方案,可用于临床环境。本研究的目的是展示通用双脉冲注射方案的设置和可行性。
使用多种不同的对比剂、对比剂剂量、动力注射器、灌注序列和 CMR 扫描仪组合来测试通用双脉冲注射方案。这包括 3 种不同的对比剂(Gd-DO3A-butrol、Gd-DTPA 和 Gd-DOTA)、4 种不同的剂量(0.025mmol/kg、0.05mmol/kg、0.075mmol/kg 和 0.1mmol/kg)、2 种不同类型的注射器(具有和不具有“暂停”功能)、5 种不同的序列(涡轮场回波(TFE)、平衡 TFE、k-空间和时间(k-t)加速 TFE、k-t 加速平衡 TFE、涡轮快速低角度拍摄)和来自 2 家不同制造商的 3 台不同的 CMR 扫描仪。获得稀释对比剂脉冲曲线的时间宽度与心输出量之间的关系,以确定稀释和浓对比剂注射之间的最佳预定义暂停时间。
共进行了 161 次双脉冲灌注扫描。观察到 3 次与注射器无关的技术错误(1.9%)。未观察到与注射器相关的错误。如果使用 0.1mmol/kg 的 Gd-DO3A-butrol 剂量,使用最佳预定义暂停,该双脉冲方案在所有参数组合中均能良好工作。线性回归分析表明,如果使用 0.1mmol/kg 的 Gd-DO3A-butrol 剂量,最佳预定义暂停时间为 25s,可分离稀释和浓对比剂脉冲曲线。
通用双脉冲注射方案不需要复杂的双头动力注射器功能,是一种可行的技术,可以获得合理的绝对 MBF 定量的动脉输入函数曲线。