Department of Internal Medicine III, Nephrology and Dialysis, Medical University of Vienna, Währinger Gürtel 18-20, Vienna 1090, Austria.
Trials. 2012 Jun 8;13:79. doi: 10.1186/1745-6215-13-79.
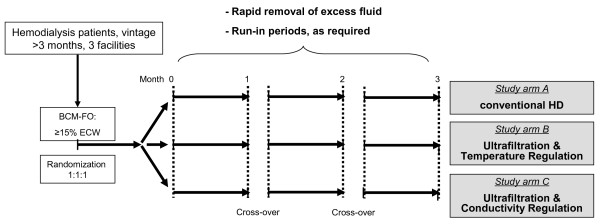
Data generated with the body composition monitor (BCM, Fresenius) show, based on bioimpedance technology, that chronic fluid overload in hemodialysis patients is associated with poor survival. However, removing excess fluid by lowering dry weight can be accompanied by intradialytic and postdialytic complications. Here, we aim at testing the hypothesis that, in comparison to conventional hemodialysis, blood volume-monitored regulation of ultrafiltration and dialysate conductivity (UCR) and/or regulation of ultrafiltration and temperature (UTR) will decrease complications when ultrafiltration volumes are systematically increased in fluid-overloaded hemodialysis patients.
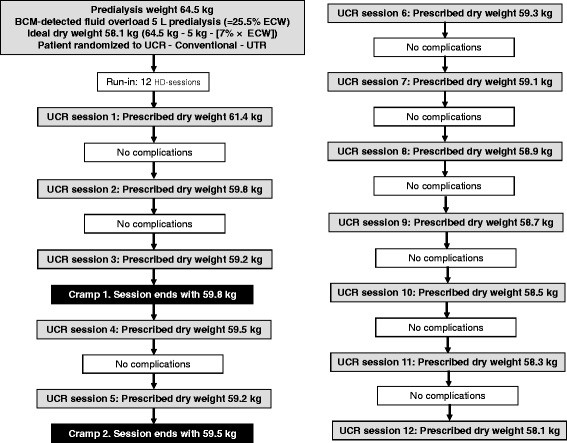
METHODS/DESIGN: BCM measurements yield results on fluid overload (in liters), relative to extracellular water (ECW). In this prospective, multicenter, triple-arm, parallel-group, crossover, randomized, controlled clinical trial, we use BCM measurements, routinely introduced in our three maintenance hemodialysis centers shortly prior to the start of the study, to recruit sixty hemodialysis patients with fluid overload (defined as ≥15% ECW). Patients are randomized 1:1:1 into UCR, UTR and conventional hemodialysis groups. BCM-determined, 'final' dry weight is set to normohydration weight -7% of ECW postdialysis, and reached by reducing the previous dry weight, in steps of 0.1 kg per 10 kg body weight, during 12 hemodialysis sessions (one study phase). In case of intradialytic complications, dry weight reduction is decreased, according to a prespecified algorithm. A comparison of intra- and post-dialytic complications among study groups constitutes the primary endpoint. In addition, we will assess relative weight reduction, changes in residual renal function, quality of life measures, and predialysis levels of various laboratory parameters including C-reactive protein, troponin T, and N-terminal pro-B-type natriuretic peptide, before and after the first study phase (secondary outcome parameters).
Patients are not requested to revert to their initial degree of fluid overload after each study phase. Therefore, the crossover design of the present study merely serves the purpose of secondary endpoint evaluation, for example to determine patient choice of treatment modality. Previous studies on blood volume monitoring have yielded inconsistent results. Since we include only patients with BCM-determined fluid overload, we expect a benefit for all study participants, due to strict fluid management, which decreases the mortality risk of hemodialysis patients.
ClinicalTrials.gov, NCT01416753.
基于生物阻抗技术,体成分监测仪(BCM,费森尤斯)生成的数据表明,慢性液体超负荷与血液透析患者的不良预后相关。然而,通过降低干体重来去除多余的液体可能会伴随透析中及透析后并发症。在这里,我们旨在检验以下假说,即在液体超负荷的血液透析患者中,与常规血液透析相比,通过监测血容量来调节超滤量和透析液电导率(UCR)和/或调节超滤量和温度(UTR),当系统地增加超滤量时,将减少并发症。
方法/设计:BCM 测量结果可提供与细胞外液(ECW)相关的液体超负荷(以升为单位)。在这项前瞻性、多中心、三臂、平行组、交叉、随机、对照临床试验中,我们使用 BCM 测量,该测量在研究开始前不久在我们的三个维持性血液透析中心常规引入,以招募 60 名液体超负荷(定义为≥15%ECW)的血液透析患者。患者按 1:1:1 随机分为 UCR、UTR 和常规血液透析组。BCM 确定的“最终”干体重设定为透析后 ECW-7%的正常水合体重,并通过在 12 次血液透析治疗中逐步减少之前的干体重(每次减少 10 公斤体重 0.1 公斤)来实现,每个研究阶段 1 次。如果发生透析中并发症,根据预设的算法减少干体重的减少。组间透析中和透析后并发症的比较构成主要终点。此外,我们将评估研究组之间的相对体重减轻、残余肾功能变化、生活质量测量以及各种实验室参数(包括 C 反应蛋白、肌钙蛋白 T 和 N 末端 pro-B 型利钠肽前体)的预透析水平,在第一个研究阶段前后(次要结果参数)。
在每个研究阶段后,患者不需要恢复到初始的液体超负荷程度。因此,本研究的交叉设计仅用于评估次要终点,例如确定患者对治疗方式的选择。以前关于血容量监测的研究结果不一致。由于我们仅包括 BCM 确定的液体超负荷患者,由于严格的液体管理,我们预计所有研究参与者都将受益,这降低了血液透析患者的死亡风险。
ClinicalTrials.gov,NCT01416753。