Department of Pathology, University of Turku, Henrikinkatu 10, Turku, 20014, Finland.
World J Surg Oncol. 2012 Jun 8;10:102. doi: 10.1186/1477-7819-10-102.
We evaluated the relationship of the apoptotic activity index (AI) and the standardized mitotic-apoptotic ratio (SMI/AI) with clinicopathological features and prognosis in Libyan female breast cancer (BC) patients. We then compared our results with corresponding results in Finnish and Nigerian female BC patients.
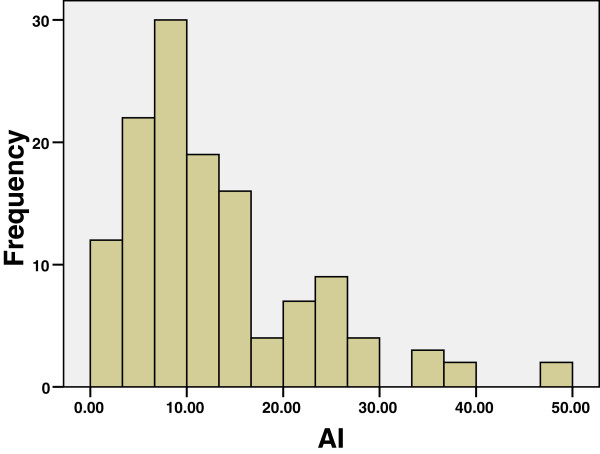
Histological samples of breast carcinoma from 130 patients were retrospectively studied: an estimation of the apoptotic activity per square millimeter (expressed as apoptotic activity index (AI)), and standardized mitotic-apoptotic ratio (SMI/AI) was made, and the results compared with the clinicopathological features and the patient's survival.
There was a statistically significant correlation between the AI and most of the clinicopathological features; the strongest association was observed for clinical stage lymph node (LN) status (P = 0.005). There were also correlations between AI and histological grade (P = 0.035), large tumor size (P = 0.011) and the clinical stage (P = 0.009). There were, however, prominent AI differences between Libyan, Nigerian and Finnish populations. The mean values of AI and SMI/AI in Libyan BC patients were 12.8 apoptotic figures per square millimeter and 2.8, respectively. The Libyan AI is slightly higher than in Nigeria, but much higher than in Finland. The differences between countries are seen throughout the samples as well as being present in certain subgroups. The survival analysis indicated that short survival time was associated with high apoptotic indices values and so can identify aggressive tumors and provide significant prognostic support. The cutoff (4 and 18 apoptosis/mm2) of AI might be applied as a quantitative criterion for Libyan BC to separate the patients into good, moderate and bad prognosis groups.
The results indicated that the differences in AI among the three countries may be due to the known variation in the distribution of genetic markers in these populations. Improvement in health care and introduction of screening programs, however, could be very helpful in the Libyan population.
我们评估了凋亡活性指数 (AI) 和标准化有丝分裂-凋亡比 (SMI/AI) 与利比亚女性乳腺癌 (BC) 患者临床病理特征和预后的关系。然后,我们将我们的结果与芬兰和尼日利亚女性 BC 患者的相应结果进行了比较。
回顾性研究了 130 例乳腺癌组织学样本:估计每平方毫米的凋亡活性(表示为凋亡活性指数 (AI)),并进行标准化有丝分裂-凋亡比 (SMI/AI),将结果与临床病理特征和患者生存情况进行比较。
AI 与大多数临床病理特征之间存在统计学显著相关性;与临床分期淋巴结 (LN) 状态的相关性最强 (P = 0.005)。AI 与组织学分级 (P = 0.035)、肿瘤体积较大 (P = 0.011) 和临床分期 (P = 0.009) 之间也存在相关性。然而,利比亚、尼日利亚和芬兰人群之间的 AI 差异显著。利比亚 BC 患者的平均 AI 和 SMI/AI 值分别为 12.8 个凋亡数/平方毫米和 2.8。利比亚的 AI 值略高于尼日利亚,但远高于芬兰。这些差异在整个样本中以及在某些亚组中均可见。生存分析表明,短生存时间与高凋亡指数值相关,因此可以识别侵袭性肿瘤并提供重要的预后支持。AI 的截止值 (4 和 18 个凋亡/毫米 2) 可作为利比亚 BC 的定量标准,将患者分为预后良好、中等和不良的组。
结果表明,三个国家之间的 AI 差异可能是由于这些人群中遗传标记分布的已知差异所致。然而,改善医疗保健和引入筛查计划可能对利比亚人口非常有帮助。