Huang Liusheng, Carey Vincent, Lindsey Jane C, Marzan Florence, Gingrich David, Graham Bobbie, Barlow-Mosha Linda, Ssemambo Phionah K, Kamthunzi Portia, Nachman Sharon, Parikh Sunil, Aweeka Francesca T
Drug Research Unit, Department of Clinical Pharmacy, University of California, San Francisco, CA, United States of America.
Center for Biostatistics in AIDS Research, Harvard TH Chan School of Public Health, Boston, MA, United States of America.
PLoS One. 2017 Oct 24;12(10):e0186589. doi: 10.1371/journal.pone.0186589. eCollection 2017.
The antiretroviral drug nevirapine and the antimalarial artemisinin-based combination therapy artemether-lumefantrine are commonly co-administered to treat malaria in the context of HIV. Nevirapine is a known inhibitor of cytochrome P450 3A4, which metabolizes artemether and lumefantrine. To address the concern that the antiretroviral nevirapine impacts the antimalarial artemether-lumefantrine pharmacokinetics, a prospective non-randomized controlled study in children presenting with uncomplicated malaria and HIV in sub-Saharan Africa was carried out.
Participants received artemether-lumefantrine (20/120 mg weight-based BID) for 3 days during nevirapine-based antiretroviral therapy (ART) co-administration (158-266 mg/m2 QD). HIV positive participants who were not yet on ART drugs were also enrolled as the control group. The target enrollment was children aged 3-12 years (n = 24 in each group). Intensive pharmacokinetics after the last artemether-lumefantrine dose was assessed for artemether, its active metabolite dihydroartemisinin, and lumefantrine. Pharmacokinetic parameters (area under the plasma concentration vs. time curve (AUC), maximum concentration and day 7 lumefantrine concentrations) were estimated using non-compartmental methods and compared to controls.
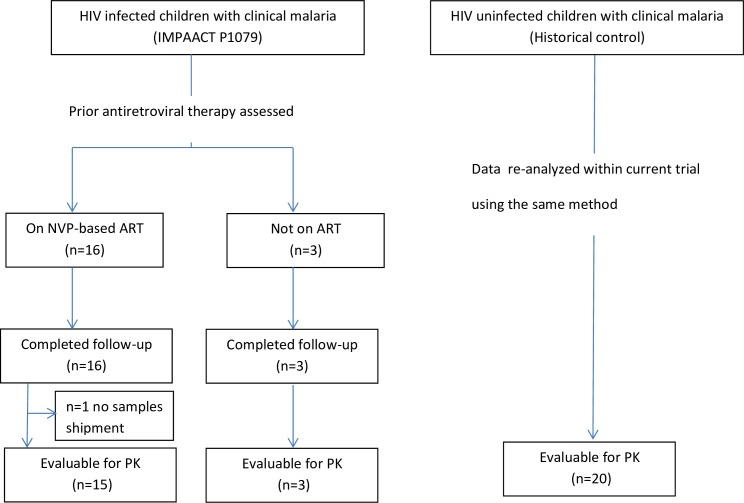
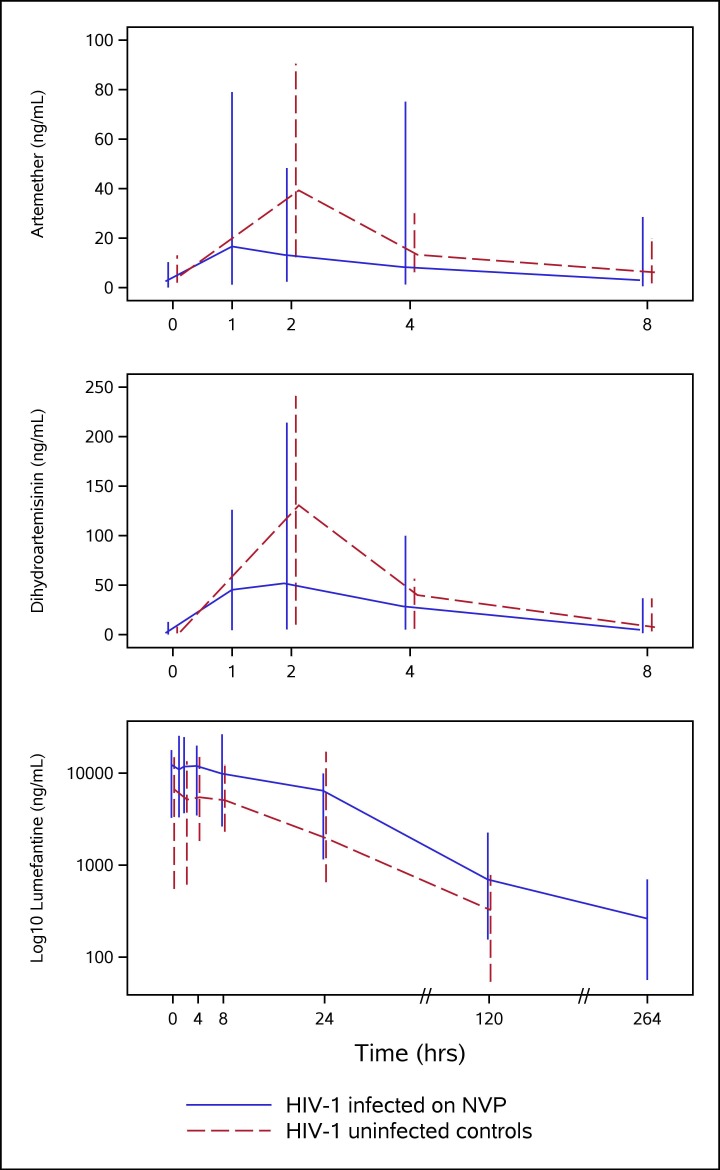
Nineteen children (16 on nevirapine and three not on ART) enrolled. Fifteen of the 16 (aged 4 to 11 years) on nevirapine-based ART were included in the pharmacokinetic analysis. Due to evolving WHO HIV treatment guidelines, insufficient children were enrolled in the control group (n = 3), so the pharmacokinetic data were compared to a historical control group of 20 HIV-uninfected children 5-12 years of age who also presented with malaria and underwent identical study procedures. Decreases of pharmacokinetic exposure [as estimated by AUC (AUC0-8hr)] were marginally significant for artemether (by -46%, p = 0.08) and dihydroartemisinin (-22%, p = 0.06) in the children on nevirapine-based ART, compared to when artemether-lumefantrine was administered alone. Similarly, peak concentration was decreased by 50% (p = 0.07) for artemether and 36% (p = 0.01) for dihydroartemisinin. In contrast, exposure to lumefantrine increased significantly in the context of nevirapine [AUC0-120hr:123% (p<0.001); Cday7:116% (p<0.001), Cmax: 95% (p<0.001)].
Nevirapine-based ART increases the exposure to lumefantrine in pre-pubescent children with a trend toward diminished artemether and dihydroartemisinin exposure. These findings contrast with other studies indicating NVP reduces or results in no change in exposure of antimalarial drugs, and may be specific to this age group (4-12 years). Considering the excellent safety profile of artemether-lumefantrine, the increase in lumefantrine is not of concern. However, the reduction in artemisinin exposure may warrant further study, and suggests that dosage adjustment of artemether-lumefantrine with nevirapine-based ART in children is likely warranted.
抗逆转录病毒药物奈韦拉平与基于青蒿素的抗疟联合疗法蒿甲醚-本芴醇通常联合使用,用于治疗合并人类免疫缺陷病毒(HIV)感染的疟疾患者。奈韦拉平是细胞色素P450 3A4的已知抑制剂,而细胞色素P450 3A4可代谢蒿甲醚和本芴醇。为解决抗逆转录病毒药物奈韦拉平影响抗疟药物蒿甲醚-本芴醇药代动力学这一问题,在撒哈拉以南非洲地区针对患有非复杂性疟疾和HIV感染的儿童开展了一项前瞻性非随机对照研究。
参与者在接受基于奈韦拉平的抗逆转录病毒治疗(ART)(158 - 266 mg/m²每日一次)的同时,接受蒿甲醚-本芴醇(按体重20/120 mg每日两次)治疗3天。尚未接受抗逆转录病毒药物治疗的HIV阳性参与者也被纳入对照组。目标入组对象为3 - 12岁儿童(每组n = 24)。在最后一剂蒿甲醚-本芴醇给药后,对蒿甲醚及其活性代谢物双氢青蒿素和本芴醇进行强化药代动力学评估。使用非房室模型方法估算药代动力学参数(血浆浓度-时间曲线下面积(AUC)、最大浓度和第7天的本芴醇浓度),并与对照组进行比较。
19名儿童入组(16名接受奈韦拉平治疗,3名未接受抗逆转录病毒治疗)。在接受基于奈韦拉平的抗逆转录病毒治疗的16名儿童(年龄4至11岁)中,有15名被纳入药代动力学分析。由于世界卫生组织(WHO)HIV治疗指南不断演变,对照组入组儿童不足(n = 3),因此将药代动力学数据与20名年龄在5 - 12岁、同样患有疟疾且接受相同研究程序的未感染HIV儿童的历史对照组进行比较。与单独使用蒿甲醚-本芴醇相比,接受基于奈韦拉平的抗逆转录病毒治疗的儿童中,蒿甲醚(AUC0 - 8小时降低46%,p = 0.08)和双氢青蒿素(降低22%,p = 0.06)的药代动力学暴露降低幅度接近显著水平。同样,蒿甲醚的峰值浓度降低了50%(p = 0.07),双氢青蒿素降低了36%(p = 0.01)。相比之下,在奈韦拉平治疗背景下,本芴醇的暴露显著增加[AUC0 - 120小时:增加123%(p<0.001);第7天浓度:增加116%(p<0.001),最大浓度:增加95%(p<0.001)]。
基于奈韦拉平的抗逆转录病毒治疗增加了青春期前儿童对本芴醇的暴露,同时蒿甲醚和双氢青蒿素的暴露有减少趋势。这些发现与其他研究结果不同,其他研究表明奈韦拉平会降低或不改变抗疟药物的暴露,可能这一结果特定于该年龄组(4 - 12岁)。鉴于蒿甲醚-本芴醇具有良好的安全性,本芴醇暴露增加并不令人担忧。然而,青蒿素暴露的减少可能需要进一步研究,这表明在儿童中,对接受基于奈韦拉平的抗逆转录病毒治疗的患者,可能需要调整蒿甲醚-本芴醇的剂量。