Formerly, Merck Rahway, NJ, USA.
Neuropsychiatr Dis Treat. 2012;8:247-57. doi: 10.2147/NDT.S29891. Epub 2012 Jun 15.
In clinical practice, clinicians often need to switch antipsychotic medications in patients with schizophrenia to optimize treatment outcomes. Here, we describe the safety and tolerability of switching existing antipsychotic treatments to asenapine or olanzapine monotherapy using various switching regimens.
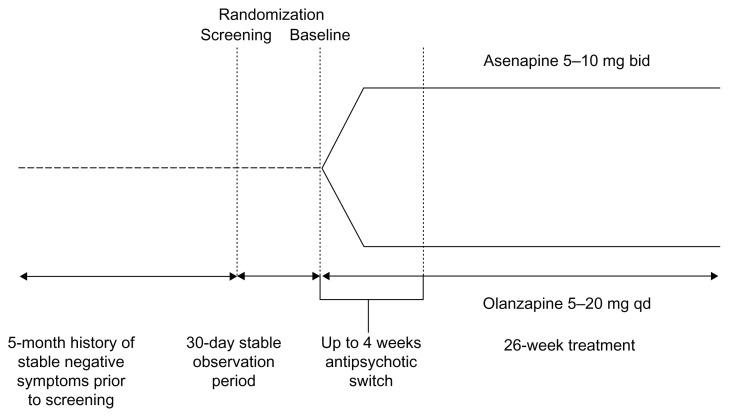
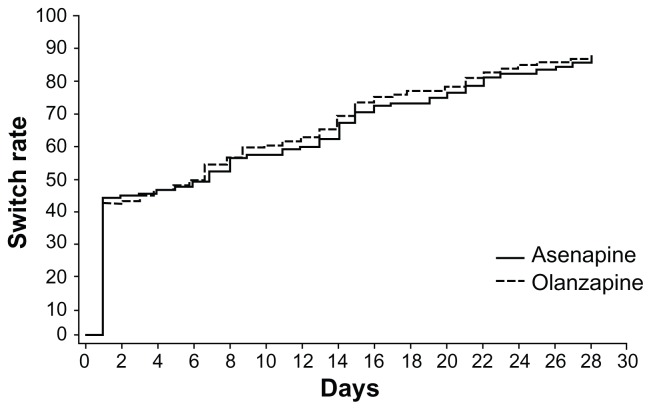
Data were pooled from 949 patients in two 26-week randomized double-blind studies. Patients with persistent negative symptoms of schizophrenia, stable for at least 5 months prior to screening and 1 additional month before randomization, were randomized to and treated with either asenapine (n = 485) or olanzapine (n = 464), and were tapered off existing antipsychotic(s) at variable rates within 28 days.
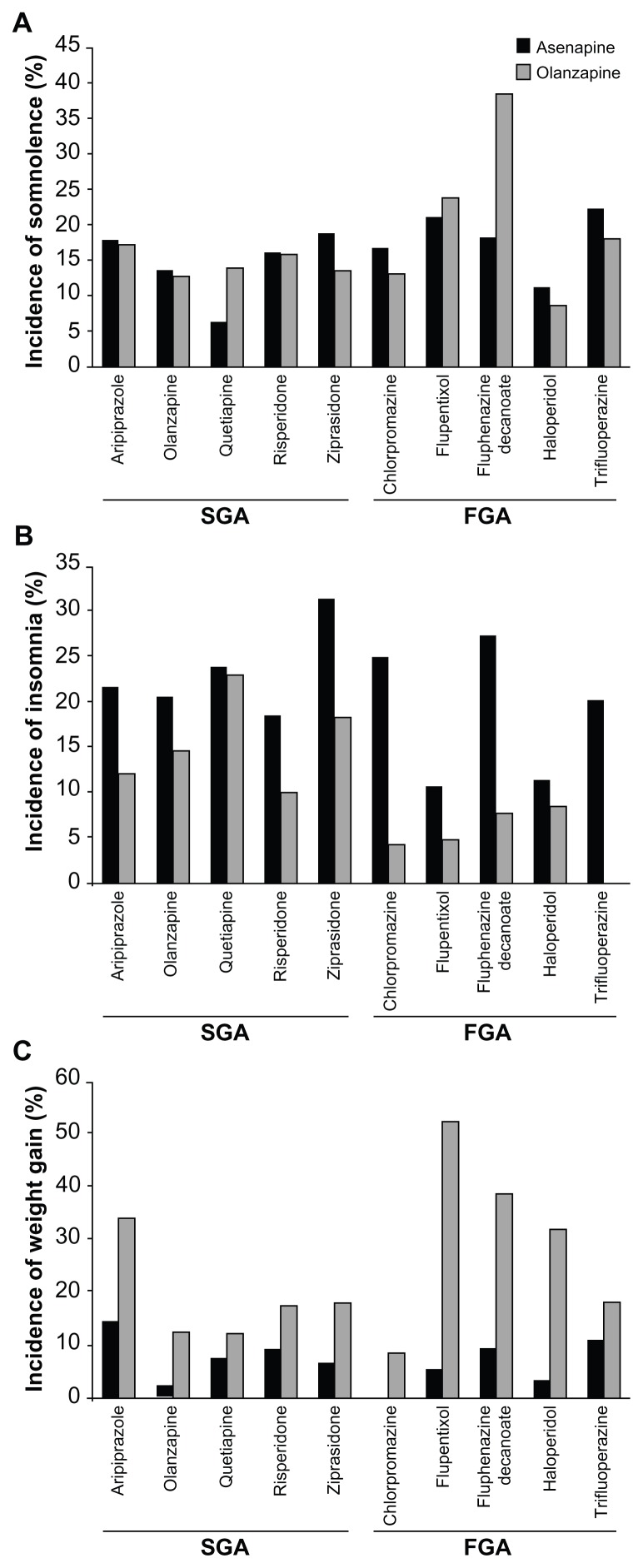
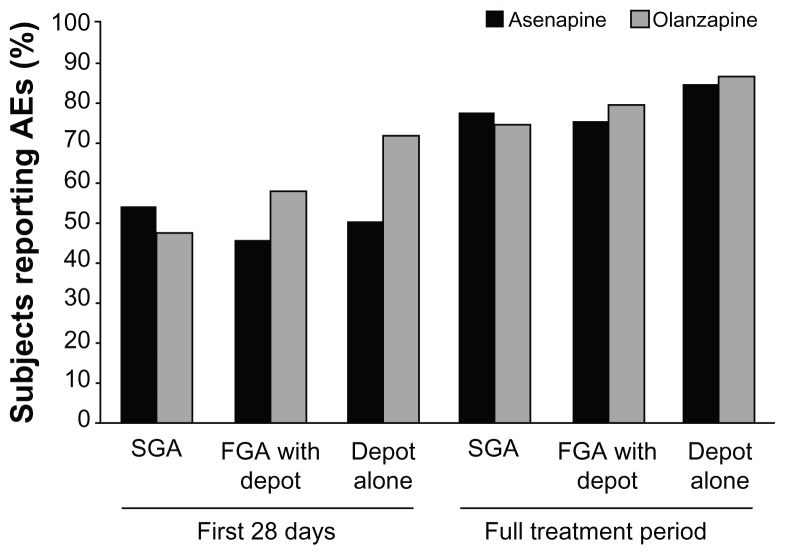
Prior to randomization, most patients were treated with second-generation antipsychotics (SGAs) (asenapine: 79.6%; olanzapine: 78.2%) and first-generation antipsychotics (FGAs) (31.1%; 29.7%), while depot formulations were used by 12.4% and 11.4%, respectively. Median time to taper off previous antipsychotics was 7 days, with approximately 40% of patients abruptly discontinuing their previous medication. Similar percentages of patients in each group reported at least one adverse event (AE) (asenapine: 76.9%; olanzapine: 75.2%). The majority of AEs occurred within the first 28 days. The most frequently reported AEs were somnolence, insomnia, and headache. The incidence of AEs in patients switching from SGAs, FGAs, or depot medications was similar between asenapine and olanzapine (77.5% vs 74.6%, 75.5% vs 79.7%, 85.0% vs 86.8%, respectively). AEs were more frequent in subjects previously treated with two antipsychotics (asenapine: 79.4%; olanzapine: 83.9%) versus one antipsychotic (asenapine: 76.3%; olanzapine: 72.2%) in the switch period.
The presented data from post hoc pooled analyses may provide practical guidance for physicians switching partially stabilized patients with schizophrenia and persistent negative symptoms to asenapine or olanzapine.
在临床实践中,临床医生经常需要为精神分裂症患者转换抗精神病药物,以优化治疗效果。在这里,我们描述了使用各种转换方案,将现有的抗精神病药物转换为阿塞那平或奥氮平单药治疗的安全性和耐受性。
数据来自两项为期 26 周的随机双盲研究中的 949 名患者。筛选前至少稳定 5 个月且在随机分组前再稳定 1 个月的持续性精神分裂症阴性症状患者,随机分为阿塞那平(n = 485)或奥氮平(n = 464)组,并在 28 天内以不同的速度逐渐停用现有的抗精神病药物。
在随机分组前,大多数患者接受第二代抗精神病药物(SGAs)(阿塞那平:79.6%;奥氮平:78.2%)和第一代抗精神病药物(FGAs)(31.1%;29.7%)治疗,同时分别有 12.4%和 11.4%的患者使用长效注射剂。之前抗精神病药物的平均停药时间为 7 天,约 40%的患者突然停止服用之前的药物。每个组中至少有 1 个不良事件(AE)报告的患者百分比相似(阿塞那平:76.9%;奥氮平:75.2%)。大多数 AE 发生在最初的 28 天内。最常报告的 AE 是嗜睡、失眠和头痛。从 SGA、FGA 或长效药物转换而来的患者中,AE 的发生率在阿塞那平和奥氮平之间相似(77.5%比 74.6%、75.5%比 79.7%、85.0%比 86.8%)。与仅使用一种抗精神病药物相比,在转换期使用两种抗精神病药物(阿塞那平:79.4%;奥氮平:83.9%)的患者中,AE 更常见(阿塞那平:76.3%;奥氮平:72.2%)。
来自事后汇总分析的数据可能为医生转换部分稳定的伴有持续性阴性症状的精神分裂症患者提供实用指导,将其转换为阿塞那平或奥氮平。