Center for Health Decision Science, Department of Health Policy and Management, Harvard School of Public Health, Boston, Massachusetts, United States of America.
PLoS One. 2012;7(6):e39555. doi: 10.1371/journal.pone.0039555. Epub 2012 Jun 22.
As part of efforts to reduce maternal deaths in Nigeria, pregnant women are being encouraged to give birth in healthcare facilities. However, little is known about whether or not available healthcare facilities can cope with an increasing demand for obstetric care. We thus carried out this survey as a rapid and tactical assessment of facility quality. We visited 121 healthcare facilities, and used the opportunity to interview over 700 women seeking care at these facilities.
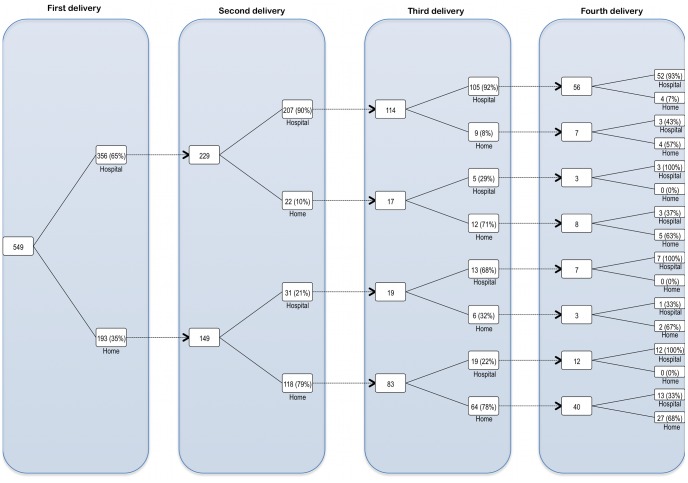
Most of the primary healthcare facilities we visited were unable to provide all basic Emergency Obstetric Care (bEmOC) services. In general, they lack clinical staff needed to dispense maternal and neonatal care services, ambulances and uninterrupted electricity supply whenever there were obstetric emergencies. Secondary healthcare facilities fared better, but, like their primary counterparts, lack neonatal care infrastructure. Among patients, most lived within 30 minutes of the visited facilities and still reported some difficulty getting there. Of those who had had two or more childbirths, the conditional probability of a delivery occurring in a healthcare facility was 0.91 if the previous delivery occurred in a healthcare facility, and 0.24 if it occurred at home. The crude risk of an adverse neonatal outcome did not significantly vary by delivery site or birth attendant, and the occurrence of such an outcome during an in-facility delivery may influence the mother to have her next delivery outside. Such an outcome during a home delivery may not prompt a subsequent in-facility delivery.
In conclusion, reducing maternal deaths in Nigeria will require attention to both increasing the number of facilities with high-quality EmOC capability and also assuring Nigerian women have access to these facilities regardless of where they live.
作为减少尼日利亚产妇死亡努力的一部分,鼓励孕妇在医疗机构分娩。然而,目前尚不清楚现有的医疗机构是否能够应对产科护理需求的增加。因此,我们进行了这项调查,作为对设施质量的快速和战术评估。我们访问了 121 家医疗机构,并借此机会采访了在这些设施寻求护理的 700 多名妇女。
我们访问的大多数初级保健设施都无法提供所有基本的紧急产科护理(bEmOC)服务。一般来说,他们缺乏提供母婴护理服务、救护车和在产科紧急情况下不间断供电所需的临床人员。二级保健设施的情况稍好一些,但与初级保健设施一样,它们缺乏新生儿护理基础设施。在患者中,大多数人居住在离就诊设施 30 分钟以内的地方,但仍报告说前往那里有些困难。在那些有两次或两次以上分娩经历的人中,如果前一次分娩是在医疗机构进行的,则在医疗机构分娩的可能性为 0.91,如果是在家中分娩的,则可能性为 0.24。新生儿不良结局的风险率并不因分娩地点或分娩人员而异,而在医疗机构分娩时发生这种结局可能会影响母亲到外面去分娩。在家庭分娩时发生这种结局可能不会促使随后在医疗机构分娩。
总之,要想在尼日利亚降低产妇死亡率,不仅需要关注增加具备高质量产科急救能力的医疗机构数量,还需要确保尼日利亚妇女无论居住在哪里都能获得这些设施。