Bouillon Kim, Sabia Severine, Jokela Markus, Gale Catharine R, Singh-Manoux Archana, Shipley Martin J, Kivimäki Mika, Batty G David
Department of Epidemiology and Public Health, University College London, 1-19 Torrington Place, London, WC1E 6BT, UK.
Age (Dordr). 2013 Aug;35(4):1457-65. doi: 10.1007/s11357-012-9446-2. Epub 2012 Jul 8.
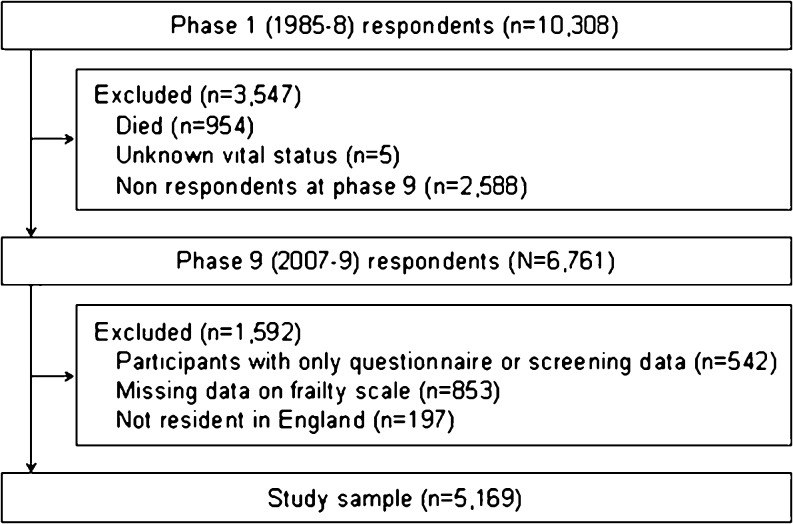
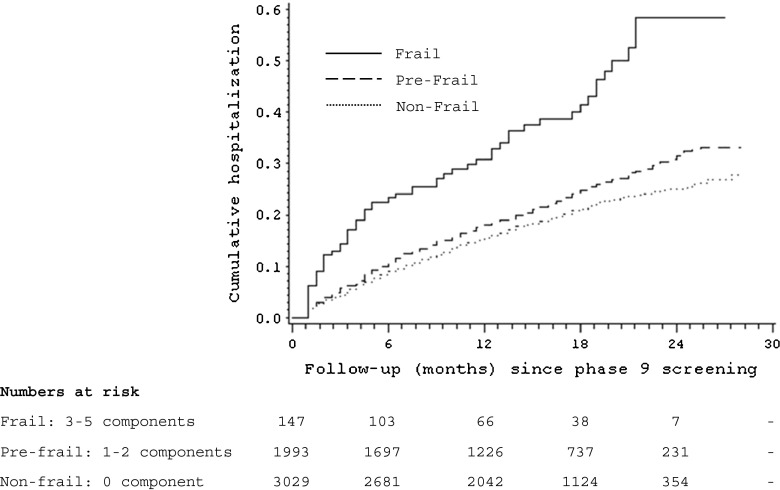
There is growing interest in the measurement of frailty in older age. The most widely used measure (Fried) characterizes this syndrome using five components: exhaustion, physical activity, walking speed, grip strength, and weight loss. These components overlap, raising the possibility of using fewer, and therefore making the device more time- and cost-efficient. The analytic sample was 5,169 individuals (1,419 women) from the British Whitehall II cohort study, aged 55 to 79 years in 2007-2009. Hospitalization data were accessed through English national records (mean follow-up 15.2 months). Age- and sex-adjusted Cox models showed that all components were significantly associated with hospitalization, the hazard ratios (HR) ranging from 1.18 (95 % confidence interval = 0.98, 1.41) for grip strength to 1.60 (1.35, 1.90) for usual walking speed. Some attenuation of these effects was apparent following mutual adjustment for frailty components, but the rank order of the strength of association remained unchanged. We observed a dose-response relationship between the number of frailty components and the risk for hospitalization [1 component-HR = 1.10 (0.96, 1.26); 2-HR = 1.52 (1.26, 1.83); 3-5-HR = 2.41 (1.84, 3.16), P trend <0.0001]. A concordance index used to evaluate the predictive power for hospital admissions of individual components and the full scale was modest in magnitude (range 0.57 to 0.58). Our results support the validity of the multi-component frailty measure, but the predictive performance of the measure is poor.
对老年人衰弱程度测量的关注日益增加。最广泛使用的测量方法(弗里德法)使用五个组成部分来描述这种综合征:疲惫、身体活动能力、步行速度、握力和体重减轻。这些组成部分相互重叠,这就增加了使用更少组成部分的可能性,从而使测量方法更节省时间和成本。分析样本来自英国白厅II队列研究中的5169名个体(1419名女性),在2007 - 2009年时年龄为55至79岁。通过英国国家记录获取住院数据(平均随访15.2个月)。年龄和性别调整后的Cox模型显示,所有组成部分都与住院显著相关,风险比(HR)范围从握力的1.18(95%置信区间 = 0.98,1.41)到通常步行速度的1.60(1.35,1.90)。在对衰弱组成部分进行相互调整后,这些效应出现了一些减弱,但关联强度的排序保持不变。我们观察到衰弱组成部分的数量与住院风险之间存在剂量反应关系[1个组成部分 - HR = 1.10(0.96,1.26);2个组成部分 - HR = 1.52(1.26,1.83);3 - 5个组成部分 - HR = 2.41(1.84,3.16),P趋势<0.0001]。用于评估各个组成部分和完整量表对住院预测能力的一致性指数大小适中(范围为0.57至0.58)。我们的结果支持多组成部分衰弱测量方法的有效性,但该测量方法的预测性能较差。