Abramson Cancer Center and the Division of Hematology and Oncology, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA 19104, USA.
N Engl J Med. 2012 Jul 12;367(2):135-45. doi: 10.1056/NEJMoa1201248.
Graft-versus-host disease (GVHD) is a major barrier to successful allogeneic hematopoietic stem-cell transplantation (HSCT). The chemokine receptor CCR5 appears to play a role in alloreactivity. We tested whether CCR5 blockade would be safe and limit GVHD in humans.
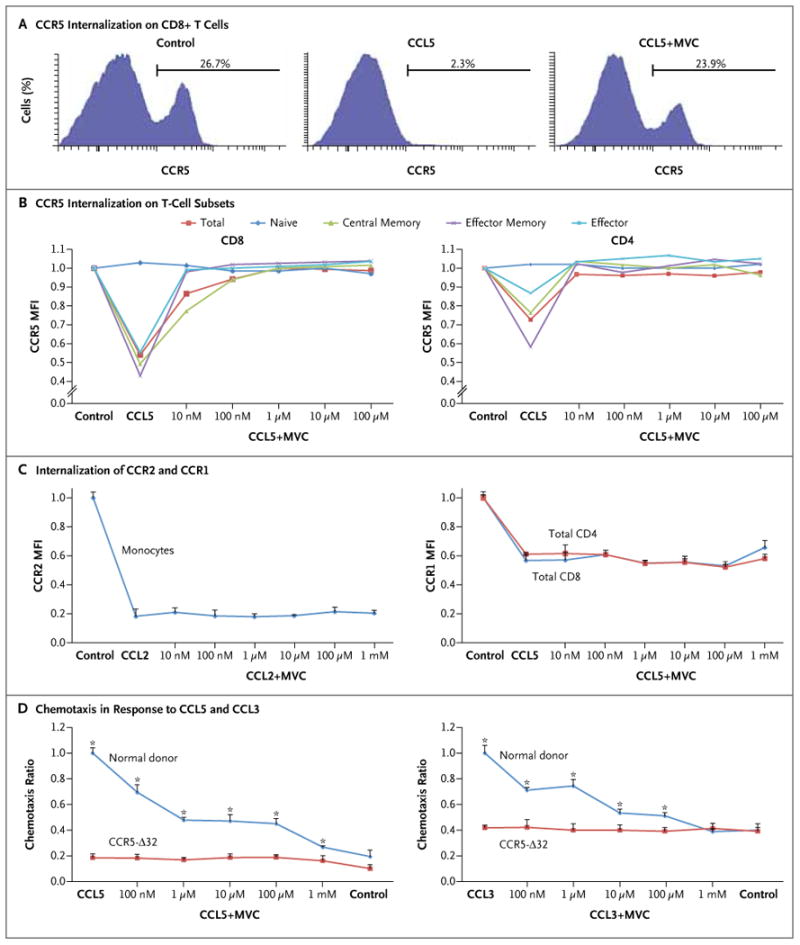
We tested the in vitro effect of the CCR5 antagonist maraviroc on lymphocyte function and chemotaxis. We then enrolled 38 high-risk patients in a single-group phase 1 and 2 study of reduced-intensity allogeneic HSCT that combined maraviroc with standard GVHD prophylaxis.
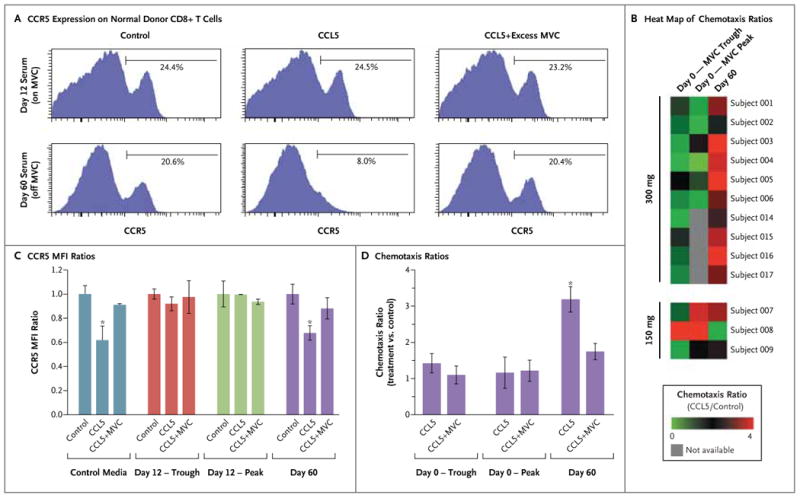
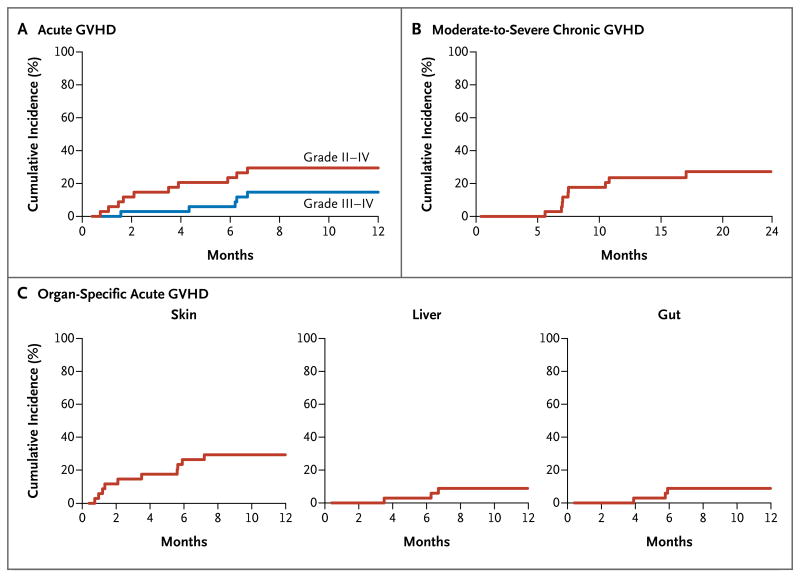
Maraviroc inhibited CCR5 internalization and lymphocyte chemotaxis in vitro without impairing T-cell function or formation of hematopoietic-cell colonies. In 35 patients who could be evaluated, the cumulative incidence rate (±SE) of grade II to IV acute GVHD was low at 14.7±6.2% on day 100 and 23.6±7.4% on day 180. Acute liver and gut GVHD were not observed before day 100 and remained uncommon before day 180, resulting in a low cumulative incidence of grade III or IV GVHD on day 180 (5.9±4.1%). The 1-year rate of death that was not preceded by disease relapse was 11.7±5.6% without excessive rates of relapse or infection. Serum from patients receiving maraviroc prevented CCR5 internalization by CCL5 and blocked T-cell chemotaxis in vitro, providing evidence of antichemotactic activity.
In this study, inhibition of lymphocyte trafficking was a specific and potentially effective new strategy to prevent visceral acute GVHD. (Funded by Pfizer and others; ClinicalTrials.gov number, NCT00948753.).
移植物抗宿主病(GVHD)是异体造血干细胞移植(HSCT)成功的主要障碍。趋化因子受体 CCR5 似乎在同种异体反应中发挥作用。我们测试了 CCR5 阻断是否安全并限制人类 GVHD。
我们测试了 CCR5 拮抗剂马拉维若在淋巴细胞功能和趋化性方面的体外作用。然后,我们对 38 名高危患者进行了一项单组 1 期和 2 期研究,该研究将马拉维若与标准 GVHD 预防相结合,进行了低强度同种异体 HSCT。
马拉维若在不损害 T 细胞功能或造血细胞集落形成的情况下,抑制 CCR5 内化和淋巴细胞趋化性。在 35 名可评估的患者中,第 100 天和第 180 天 2 至 4 级急性 GVHD 的累积发生率(±SE)分别为 14.7±6.2%和 23.6±7.4%。第 100 天之前未观察到急性肝和肠道 GVHD,第 180 天之前仍不常见,导致第 180 天 3 或 4 级 GVHD 的累积发生率低(5.9±4.1%)。无疾病复发的 1 年死亡率为 11.7±5.6%,复发或感染率不高。接受马拉维若的患者的血清可阻止 CCL5 内化 CCR5,并在体外阻断 T 细胞趋化性,这提供了抗趋化活性的证据。
在这项研究中,抑制淋巴细胞迁移是一种预防内脏急性 GVHD 的特异性且潜在有效的新策略。(由辉瑞等资助;临床试验.gov 编号,NCT00948753)。