Abramson Cancer Center and Division of Hematology/Oncology, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, Pennsylvania; Division of Hematology/Oncology and Columbia Center for Translational Immunology, Department of Medicine, Columbia University Medical Center, New York, New York.
Abramson Cancer Center and Division of Hematology/Oncology, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, Pennsylvania.
Biol Blood Marrow Transplant. 2019 Mar;25(3):515-521. doi: 10.1016/j.bbmt.2018.09.034. Epub 2018 Oct 10.
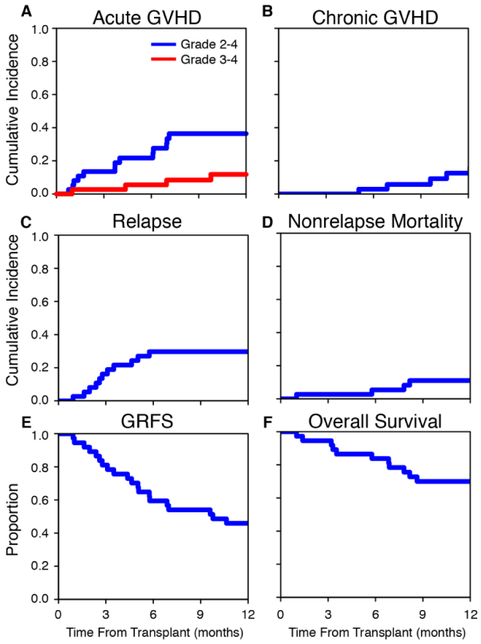
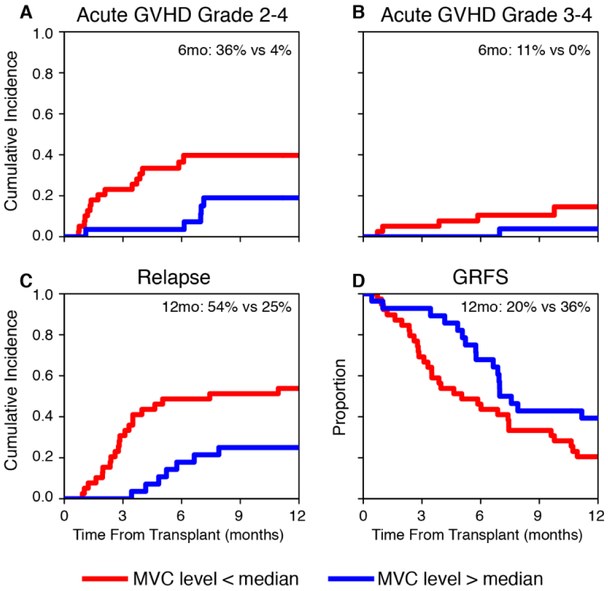
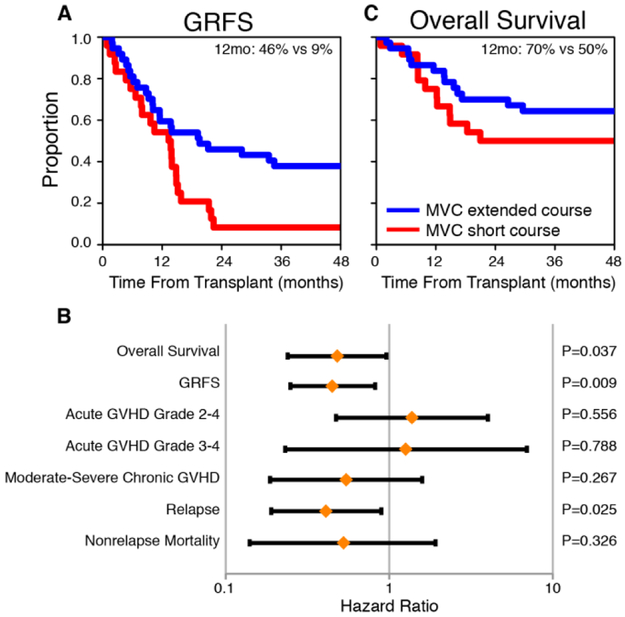
Graft-versus-host disease (GVHD) remains the most common treatment-related complication after allogeneic hematopoietic cell transplantation (allo-HCT). Lymphocyte migration plays a critical role in the pathogenesis of GVHD. A previous phase I/II trial demonstrated that CCR5 blockade with maraviroc in the first 30days after allo-HCT resulted in a low incidence of early acute GVHD, primarily in visceral organs, but with no impact on late acute or chronic GVHD. We conducted a phase II trial to examine the efficacy of an extended course of maraviroc, administered through post-transplantation day +90 in addition to standard prophylaxis in 37 recipients of reduced-intensity-conditioned unrelated donor allo-HCT performed to treat hematologic malignancies. Extended maraviroc treatment was safe and feasible. The primary study endpoint, day +180 rate of grade II-IV acute GVHD, was 22 ± 7%, liver GVHD was not observed, and gut GVHD was uncommon. The day +180 rate of grade III-IV acute GVHD was 5 ± 4%. The 1-year rate of moderate to severe chronic GVHD was 8 ± 5% and that of disease relapse was 30 ± 8%. Overall survival at 1 year was 70 ± 8%. Compared with the previously studied short course of maraviroc, the extended course resulted in a significantly higher GVHD-free, relapse-free survival (adjusted hazard ratio [HR], .45; 95% confidence interval [CI], .25 to .82; P = .009) and overall survival (adjusted HR, .48; 95% CI, .24 to .96; P = .037). A combined analysis of both trials showed that high maraviroc trough concentrations on the day of hematopoietic cell infusion were associated with lower rates of acute GVHD. An extended course of maraviroc after reduced-intensity-conditioned unrelated donor allo-HCT is safe and effective in preventing acute and chronic GVHD and is associated with favorable survival.
移植物抗宿主病(GVHD)仍然是异基因造血细胞移植(allo-HCT)后最常见的治疗相关并发症。淋巴细胞迁移在 GVHD 的发病机制中起着关键作用。一项先前的 I/II 期试验表明,allo-HCT 后 30 天内用马拉维若治疗 CCR5 阻断导致早期急性 GVHD 的发生率较低,主要是内脏器官,但对晚期急性或慢性 GVHD 没有影响。我们进行了一项 II 期试验,以检查在 37 名接受减强度非亲缘供体 allo-HCT 治疗血液恶性肿瘤的患者中,在移植后第+90 天加用标准预防方案的情况下,延长马拉维若治疗时间的疗效。延长马拉维若治疗是安全可行的。主要研究终点为第+180 天 II-IV 级急性 GVHD 的发生率为 22±7%,未观察到肝 GVHD,且肠道 GVHD 不常见。第+180 天 III-IV 级急性 GVHD 的发生率为 5±4%。1 年时中重度慢性 GVHD 的发生率为 8±5%,疾病复发率为 30±8%。1 年总生存率为 70±8%。与之前研究的短程马拉维若相比,延长疗程导致 GVHD 无复发、无复发生存(调整后的危险比[HR],.45;95%置信区间[CI],.25 至.82;P=0.009)和总生存(调整后的 HR,.48;95%CI,.24 至.96;P=0.037)显著提高。两项试验的联合分析表明,造血细胞输注当天马拉维若的低浓度与急性 GVHD 发生率降低有关。在减强度非亲缘供体 allo-HCT 后延长马拉维若的疗程可安全有效地预防急性和慢性 GVHD,并与良好的生存相关。