Seiki Stephanie, Chonchol Michel, Cheung Alfred K, Kaufman James S, Greene Tom, Roberts William L, Smits Gerard, Kendrick Jessica
Division of Renal Diseases and Hypertension, University of Colorado School of Medicine, Aurora, CO 80204, USA.
Clin Nephrol. 2012 Dec;78(6):432-41. doi: 10.5414/CN107498.
Patients with chronic kidney disease (CKD) not requiring dialysis have a high prevalence of 25-hydroxyvitamin D (25(OH)D) deficiency but the relationship between 25(OH)D levels and metabolic syndrome is unknown in this population.
This study analyzed stored plasma samples from 495 non-diabetic subjects with severe kidney disease, not yet on dialysis, who participated in the homocysteine in kidney and end stage renal disease study. Metabolic syndrome was defined as the presence of all three of the following: (1) Serum triglycerides ≥ 150 mg/dl or drug treatment for hypertriglyceridemia; (2) serum high density lipoprotein-cholesterol (HDL-C) < 50 mg/dl for women or < 40 mg/dl for men or drug treatment for dyslipidemia; and (3) blood pressure ≥ 130/85 mmHg or drug treatment for hypertension. Multivariate logistic regression models were used to evaluate the cross-sectional association between plasma 25(OH)D levels and metabolic syndrome.
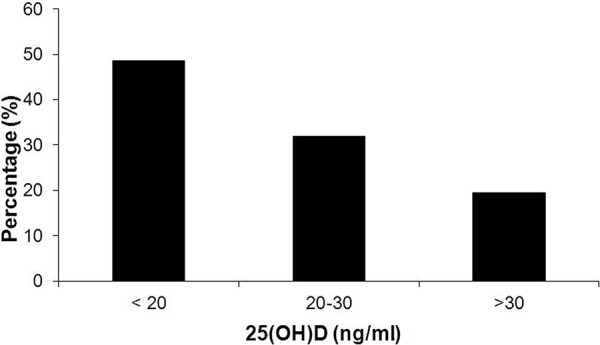
The prevalence of metabolic syndrome increased as 25(OH)D levels declined, with the highest prevalence in participants with 25(OH)D levels < 20 ng/ ml. Participants with 25(OH)D levels < 20 ng/ml had a significantly increased risk of metabolic syndrome compared to subjects with levels > 30 ng/ml after adjustment for multiple confounders (OR 2.25, 95% CI 1.25 - 4.07). Plasma 25(OH)D levels were inversely associated with diastolic blood pressure (R = -0.10, p = 0.029) and serum triglyceride levels (R = -0.14, p = 0.002).
25(OH)D deficiency is strongly associated with an increased risk of metabolic syndrome in non-diabetic patients with severe CKD not yet on dialysis, independent of cardiometabolic risk factors and other important regulators of mineral metabolism.
不需要透析的慢性肾脏病(CKD)患者中,25-羟维生素D(25(OH)D)缺乏症的患病率很高,但在该人群中,25(OH)D水平与代谢综合征之间的关系尚不清楚。
本研究分析了495名患有严重肾脏疾病且尚未接受透析的非糖尿病受试者的储存血浆样本,这些受试者参与了肾脏和终末期肾病中的同型半胱氨酸研究。代谢综合征的定义为存在以下所有三项:(1)血清甘油三酯≥150mg/dl或接受高甘油三酯血症药物治疗;(2)女性血清高密度脂蛋白胆固醇(HDL-C)<50mg/dl或男性<40mg/dl或接受血脂异常药物治疗;(3)血压≥130/85mmHg或接受高血压药物治疗。使用多变量逻辑回归模型评估血浆25(OH)D水平与代谢综合征之间的横断面关联。
随着25(OH)D水平下降,代谢综合征的患病率增加,25(OH)D水平<20ng/ml的参与者患病率最高。在调整多个混杂因素后,25(OH)D水平<20ng/ml的参与者与水平>30ng/ml的受试者相比,代谢综合征风险显著增加(比值比2.25,95%置信区间1.25 - 4.07)。血浆25(OH)D水平与舒张压(R = -0.10,p = 0.029)和血清甘油三酯水平(R = -0.14,p = 0.002)呈负相关。
在尚未接受透析的严重CKD非糖尿病患者中,25(OH)D缺乏与代谢综合征风险增加密切相关,独立于心血管代谢危险因素和矿物质代谢的其他重要调节因子。