Laboratory of Clinical Pharmacology and Therapeutics, Faculty of Medicine, University of Lisbon.
BMJ. 2012 Jul 11;345:e4260. doi: 10.1136/bmj.e4260.
To systematically review longitudinal studies evaluating use of angiotensin converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs) and risk of pneumonia.
Systematic review and meta-analysis.
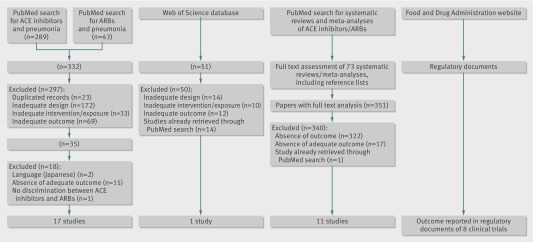
Medline through PubMed, Web of Science with conference proceedings (inception to June 2011), and US Food and Drug Administration website (June 2011). Systematic reviews and references of retrieved articles were also searched.
Two reviewers independently selected randomised controlled trials and cohort and case-control studies evaluating the use of ACE inhibitors or ARBs and risk of pneumonia and retrieved characteristics of the studies and data estimates.
The primary outcome was incidence of pneumonia and the secondary outcome was pneumonia related mortality. Subgroup analyses were carried according to baseline morbidities (stroke, heart failure, and chronic kidney disease) and patients' characteristics (Asian and non-Asian). Pooled estimates of odds ratios and 95% confidence intervals were derived by random effects meta-analysis. Adjusted frequentist indirect comparisons between ACE inhibitors and ARBs were estimated and combined with direct evidence whenever available. Heterogeneity was assessed using the I(2) test.
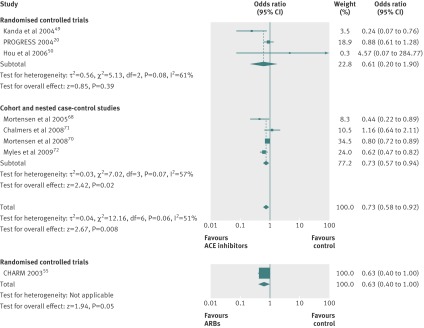
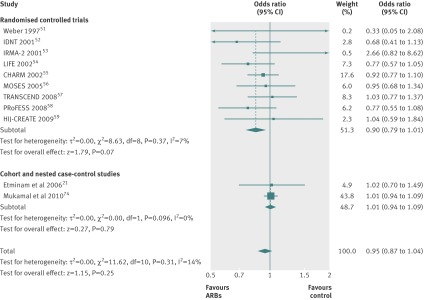
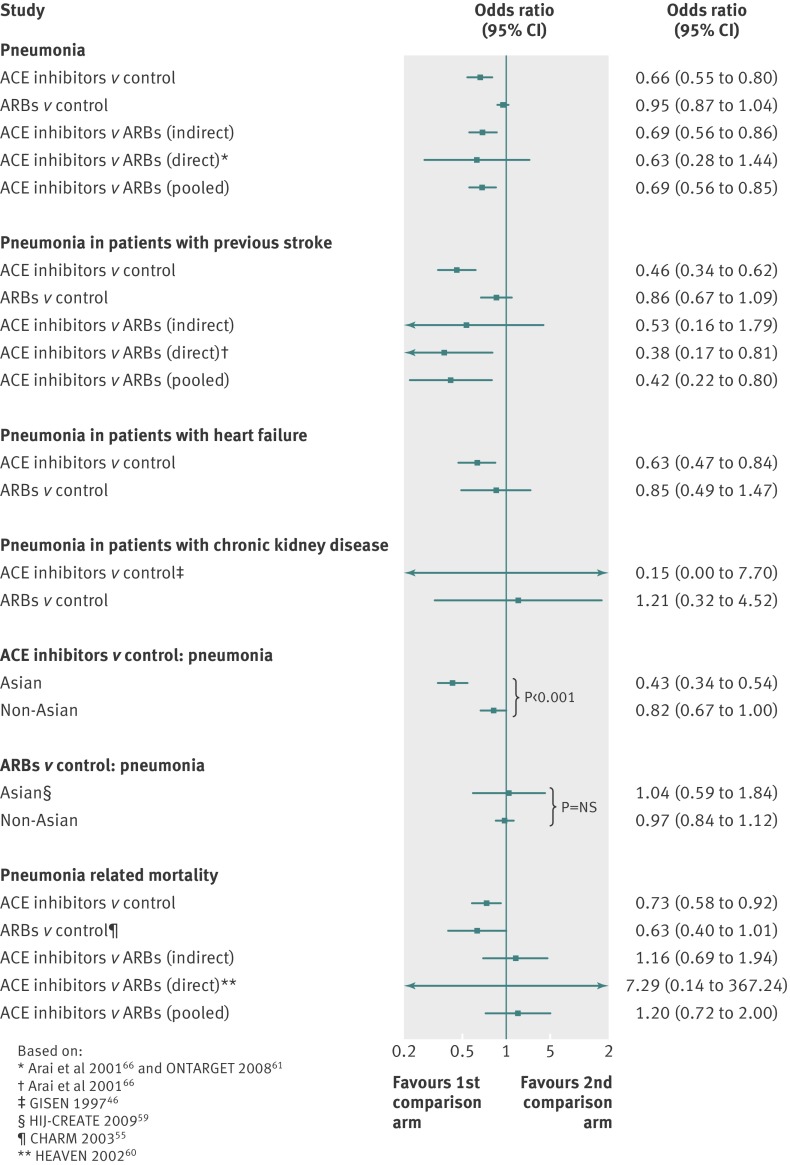
37 eligible studies were included. ACE inhibitors were associated with a significantly reduced risk of pneumonia compared with control treatment (19 studies: odds ratio 0.66, 95% confidence interval 0.55 to 0.80; I(2) = 79%) and ARBs (combined direct and indirect odds ratio estimate 0.69, 0.56 to 0.85). In patients with stroke, the risk of pneumonia was also lower in those treated with ACE inhibitors compared with control treatment (odds ratio 0.46, 0.34 to 0.62) and ARBs (0.42, 0.22 to 0.80). ACE inhibitors were associated with a significantly reduced risk of pneumonia among Asian patients (0.43, 0.34 to 0.54) compared with non-Asian patients (0.82, 0.67 to 1.00; P<0.001). Compared with control treatments, both ACE inhibitors (seven studies: odds ratio 0.73, 0.58 to 0.92; I(2)=51%) and ARBs (one randomised controlled trial: 0.63, 0.40 to 1.00) were associated with a decrease in pneumonia related mortality, without differences between interventions.
The best evidence available points towards a putative protective role of ACE inhibitors but not ARBs in risk of pneumonia. Patient populations that may benefit most are those with previous stroke and Asian patients. ACE inhibitors were also associated with a decrease in pneumonia related mortality, but the data lacked strength.
系统回顾评估血管紧张素转换酶(ACE)抑制剂或血管紧张素受体阻滞剂(ARB)使用与肺炎风险的纵向研究。
系统评价和荟萃分析。
PubMed 中的 Medline、包含会议录的 Web of Science(从创刊到 2011 年 6 月)和美国食品和药物管理局网站(2011 年 6 月)。还检索了检索到的文章的系统评价和参考文献。
两名评审员独立选择了评估 ACE 抑制剂或 ARB 使用与肺炎风险的随机对照试验和队列及病例对照研究,并检索了研究特征和数据估计值。
主要结局是肺炎的发生率,次要结局是肺炎相关死亡率。根据基线合并症(中风、心力衰竭和慢性肾脏病)和患者特征(亚洲人和非亚洲人)进行亚组分析。通过随机效应荟萃分析得出比值比和 95%置信区间的综合估计值。在有条件时,通过估计 ACE 抑制剂和 ARB 之间的调整后似然间接比较并结合直接证据进行综合。使用 I(2)检验评估异质性。
纳入 37 项符合条件的研究。与对照治疗相比,ACE 抑制剂与肺炎风险显著降低相关(19 项研究:比值比 0.66,95%置信区间 0.55 至 0.80;I(2)=79%)和 ARB(联合直接和间接比值比估计值 0.69,0.56 至 0.85)。在中风患者中,与对照治疗相比,ACE 抑制剂治疗的肺炎风险也更低(比值比 0.46,0.34 至 0.62)和 ARB(0.42,0.22 至 0.80)。与非亚洲患者(0.82,0.67 至 1.00;P<0.001)相比,ACE 抑制剂在亚洲患者中与肺炎风险降低显著相关(0.43,0.34 至 0.54)。与对照治疗相比,ACE 抑制剂(7 项研究:比值比 0.73,0.58 至 0.92;I(2)=51%)和 ARB(1 项随机对照试验:0.63,0.40 至 1.00)均与肺炎相关死亡率降低相关,干预措施之间无差异。
目前最佳证据表明 ACE 抑制剂而非 ARB 可能具有降低肺炎风险的作用。可能从治疗中获益最大的患者人群是既往有中风和亚洲患者。ACE 抑制剂还与肺炎相关死亡率降低相关,但数据强度不足。