Gammelager Henrik, Christiansen Christian Fynbo, Johansen Martin Berg, Tønnesen Else, Jespersen Bente, Sørensen Henrik Toft
Crit Care. 2012 Jul 12;16(4):R124. doi: 10.1186/cc11420.
There are few studies on long-term mortality among intensive care unit (ICU) patients with acute kidney injury (AKI). We assessed the prevalence of AKI at ICU admission, its impact on mortality during one year of follow-up, and whether the influence of AKI varied in subgroups of ICU patients.
We identified all adults admitted to any ICU in Northern Denmark (approximately 1.15 million inhabitants) from 2005 through 2010 using population-based medical registries. AKI was defined at ICU admission based on the risk, injury, failure, loss of kidney function, and end-stage kidney disease (RIFLE) classification, using plasma creatinine changes. We included four severity levels: AKI-risk, AKI-injury, AKI-failure, and without AKI. We estimated cumulative mortality by the Kaplan-Meier method and hazard ratios (HRs) using a Cox model adjusted for potential confounders. We computed estimates for all ICU patients and for subgroups with different comorbidity levels, chronic kidney disease status, surgical status, primary hospital diagnosis, and treatment with mechanical ventilation or with inotropes/vasopressors.
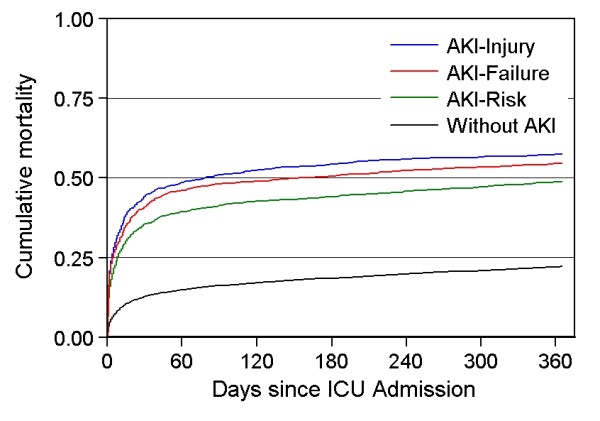
We identified 30,762 ICU patients, of which 4,793 (15.6%) had AKI at ICU admission. Thirty-day mortality was 35.5% for the AKI-risk group, 44.2% for the AKI-injury group, and 41.0% for the AKI-failure group, compared with 12.8% for patients without AKI. The corresponding adjusted HRs were 1.96 (95% confidence interval (CI) 1.80-2.13), 2.60 (95% CI 2.38 to 2.85) and 2.41 (95% CI 2.21 to 2.64), compared to patients without AKI. Among patients surviving 30 days (n = 25,539), 31- to 365 day mortality was 20.5% for the AKI-risk group, 23.8% for the AKI-injury group, and 23.2% for the AKI-failure group, compared with 10.7% for patients without AKI, corresponding to adjusted HRs of 1.33 (95% CI 1.17 to 1.51), 1.60 (95% CI 1.37 to1.87), and 1.64 (95% CI 1.42 to 1.90), respectively. The association between AKI and 30-day mortality was evident in subgroups of the ICU population, with associations persisting in most subgroups during the 31- to 365-day follow-up period, although to a lesser extent than for the 30-day period.
AKI at ICU admission is an important prognostic factor for mortality throughout the subsequent year.
关于急性肾损伤(AKI)的重症监护病房(ICU)患者的长期死亡率的研究较少。我们评估了ICU入院时AKI的患病率、其对一年随访期间死亡率的影响,以及AKI的影响在ICU患者亚组中是否存在差异。
我们使用基于人群的医疗登记系统,确定了2005年至2010年期间丹麦北部任何ICU收治的所有成年人(约115万居民)。根据风险、损伤、衰竭、肾功能丧失和终末期肾病(RIFLE)分类,利用血浆肌酐变化在ICU入院时定义AKI。我们纳入了四个严重程度级别:AKI风险、AKI损伤、AKI衰竭和无AKI。我们使用Kaplan-Meier方法估计累积死亡率,并使用针对潜在混杂因素进行调整的Cox模型估计风险比(HR)。我们计算了所有ICU患者以及不同合并症水平、慢性肾病状态、手术状态、主要医院诊断以及接受机械通气或使用血管活性药物治疗的亚组的估计值。
我们确定了30762例ICU患者,其中4793例(15.6%)在ICU入院时患有AKI。AKI风险组的30天死亡率为35.5%,AKI损伤组为44.2%,AKI衰竭组为41.0%,而无AKI患者为12.8%。与无AKI患者相比,相应的调整后HR分别为1.96(95%置信区间(CI)1.80 - 2.13)、2.60(95% CI 2.38至2.85)和2.41(95% CI 2.21至2.64)。在存活30天的患者(n = 25539)中,AKI风险组的31至365天死亡率为20.5%,AKI损伤组为23.8%,AKI衰竭组为23.2%,而无AKI患者为10.7%,相应的调整后HR分别为1.33(95% CI 1.17至1.51)、1.60(95% CI 1.37至1.87)和1.64(95% CI 1.42至1.90)。AKI与30天死亡率之间的关联在ICU人群亚组中很明显,在31至365天的随访期间,大多数亚组中这种关联仍然存在,尽管程度低于30天期间。
ICU入院时的AKI是随后一年死亡率的重要预后因素。