Kenya Medical Research Institute/Center for Disease Control Research and Public Health Collaboration, Kisumu, Kenya.
PLoS One. 2012;7(7):e38691. doi: 10.1371/journal.pone.0038691. Epub 2012 Jul 6.
We conducted a tuberculosis (TB) prevalence survey and evaluated the screening methods used in our survey, to assess if screening in TB prevalence surveys could be simplified, and to assess the accuracy of screening algorithms that may be applicable for active case finding.
All participants with a positive screen on either a symptom questionnaire, chest radiography (CXR) and/or sputum smear microscopy submitted sputum for culture. HIV status was obtained from prevalent cases. We estimated the accuracy of modified screening strategies with bacteriologically confirmed TB as the gold standard, and compared these with other survey reports. We also assessed whether sequential rather than parallel application of symptom, CXR and HIV screening would substantially reduce the number of participants requiring CXR and/or sputum culture.
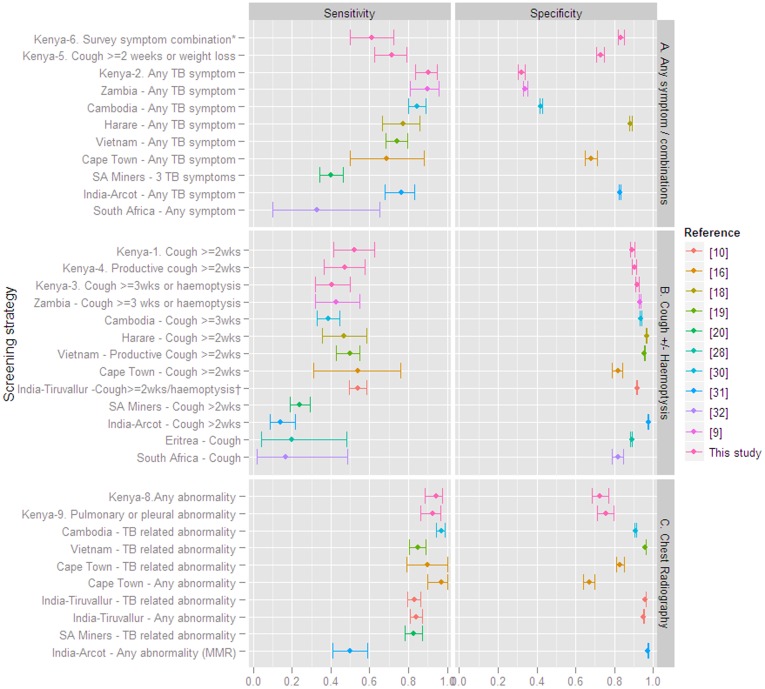
Presence of any abnormality on CXR had 94% (95%CI 88-98) sensitivity (92% in HIV-infected and 100% in HIV-uninfected) and 73% (95%CI 68-77) specificity. Symptom screening combinations had significantly lower sensitivity than CXR except for 'any TB symptom' which had 90% (95%CI 84-95) sensitivity (96% in HIV-infected and 82% in HIV-uninfected) and 32% (95%CI 30-34) specificity. Smear microscopy did not yield additional suspects, thus the combined symptom/CXR screen applied in the survey had 100% (95%CI 97-100) sensitivity. Specificity was 65% (95%CI 61-68). Sequential application of first a symptom screen for 'any symptom', followed by CXR-evaluation and different suspect criteria depending on HIV status would result in the largest reduction of the need for CXR and sputum culture, approximately 36%, but would underestimate prevalence by 11%.
CXR screening alone had higher accuracy compared to symptom screening alone. Combined CXR and symptom screening had the highest sensitivity and remains important for suspect identification in TB prevalence surveys in settings where bacteriological sputum examination of all participants is not feasible.
我们进行了一次结核病(TB)患病率调查,并评估了我们调查中使用的筛查方法,以评估筛查是否可以简化,以及评估可能适用于活动性病例发现的筛查算法的准确性。
所有在症状问卷、胸部 X 光(CXR)和/或痰涂片显微镜检查中任一检查呈阳性的参与者都提交了痰培养。从现患病例中获得 HIV 状态。我们以细菌学确诊的 TB 为金标准,估计了改良筛查策略的准确性,并与其他调查报告进行了比较。我们还评估了是否依次而不是平行应用症状、CXR 和 HIV 筛查,是否可以大大减少需要进行 CXR 和/或痰培养的参与者数量。
CXR 上存在任何异常的敏感性为 94%(95%CI 88-98)(HIV 感染者为 92%,HIV 未感染者为 100%),特异性为 73%(95%CI 68-77)。除了“任何 TB 症状”(HIV 感染者为 90%(95%CI 84-95),HIV 未感染者为 82%),症状筛查组合的敏感性明显低于 CXR,特异性为 32%(95%CI 30-34)。涂片显微镜检查没有发现更多的可疑病例,因此,在调查中应用的联合症状/CXR 筛查具有 100%(95%CI 97-100)的敏感性。特异性为 65%(95%CI 61-68)。首先进行“任何症状”的症状筛查,然后根据 HIV 状态进行 CXR 评估和不同的可疑标准的顺序应用,将导致对 CXR 和痰培养的需求减少约 36%,但会低估患病率 11%。
与单独进行症状筛查相比,CXR 筛查具有更高的准确性。联合 CXR 和症状筛查具有最高的敏感性,对于在无法对所有参与者进行细菌学痰检查的情况下进行结核病患病率调查中的可疑病例识别仍然很重要。