Hosokawa Isamu, Kato Atsushi, Shimizu Hiroaki, Furukawa Katsunori, Miyazaki Masaru
Department of General Surgery, Chiba University Graduate School of Medicine, 1-8-1 Inohana, Chuo-ku, Chiba, 260-8670, Japan.
J Med Case Rep. 2012 Jul 16;6:198. doi: 10.1186/1752-1947-6-198.
Malignant afferent loop obstruction following pancreaticoduodenectomy is a rare complication and may be fatal if suppurative cholangitis or obstructive jaundice develops. Effective and safe therapeutic strategies for malignant afferent loop obstruction following pancreaticoduodenectomy are scarce at present.
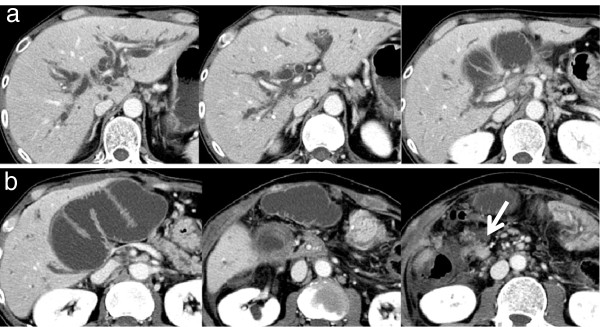
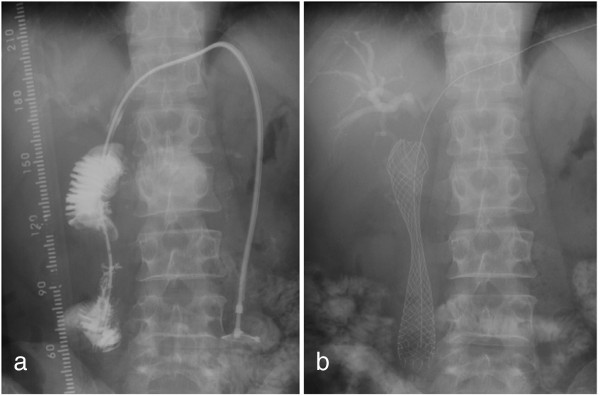
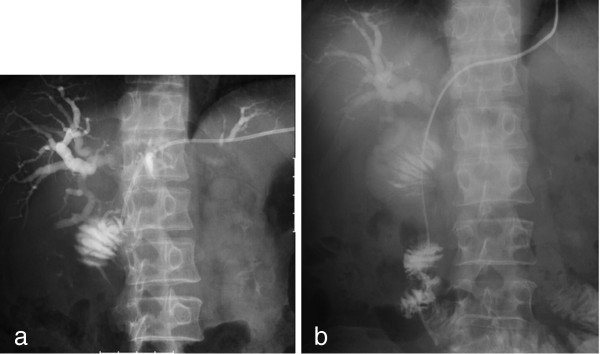
A 51-year-old Japanese man underwent pancreaticoduodenectomy for carcinoma of the papilla of Vater. Seven months postoperatively, he developed a high-grade fever, jaundice, and right upper abdominal pain. Abdominal contrast-enhanced computed tomography showed afferent loop obstruction and intrahepatic bile duct dilatation due to nodal recurrence. Percutaneous transhepatic biliary drainage was performed, and a self-expanding metallic stent (WallFlex™ duodenal stent) was placed across the stricture using the transhepatic route.
There are surgical and nonsurgical treatments for malignant afferent loop obstruction following pancreaticoduodenectomy. Nonsurgical treatments include either an endoscopic or percutaneous approach to the afferent loop. Of these methods, percutaneous transhepatic insertion of a self-expanding metallic stent is the preferred treatment for malignant afferent loop obstruction following pancreaticoduodenectomy because it is more prompt and less invasive.
胰十二指肠切除术后恶性输入袢梗阻是一种罕见的并发症,如果发生化脓性胆管炎或梗阻性黄疸可能会致命。目前,针对胰十二指肠切除术后恶性输入袢梗阻的有效且安全的治疗策略较为匮乏。
一名51岁的日本男性因 Vater 乳头癌接受了胰十二指肠切除术。术后7个月,他出现高热、黄疸和右上腹疼痛。腹部增强计算机断层扫描显示因淋巴结复发导致输入袢梗阻和肝内胆管扩张。进行了经皮经肝胆道引流,并通过经肝途径在狭窄处放置了自膨式金属支架(WallFlex™十二指肠支架)。
胰十二指肠切除术后恶性输入袢梗阻有手术和非手术治疗方法。非手术治疗包括对输入袢采用内镜或经皮途径。在这些方法中,经皮经肝插入自膨式金属支架是胰十二指肠切除术后恶性输入袢梗阻的首选治疗方法,因为它更迅速且侵入性更小。