Leue Carsten, Buijs Servaas, Strik Jacqueline, Lousberg Richel, Smit Jasper, van Kleef Maarten, van Os Jim
Department of Psychiatry and Psychology, South Limburg Mental Health Research and Teaching Network, EURON, Maastricht University Medical Centre, Maastricht, The Netherlands.
BMJ Open. 2012 Jul 19;2(4). doi: 10.1136/bmjopen-2011-000731. Print 2012.
To examine, in the light of the association between urban environment and poor mental health, whether urbanisation and neighbourhood deprivation are associated with analgesic escalation in chronic pharmacological pain treatment and whether escalation is associated with prescriptions of psychotropic medication.
Longitudinal analysis of a population-based routine dispensing database in the Netherlands.
Representative sample of pharmacies, covering 73% of the Dutch nationwide medication consumption in the primary care and hospital outpatient settings.
449 410 patients aged 15-85 years were included, of whom 166 374 were in the Starter group and 283 036 in the Continuation group of chronic analgesic treatment.
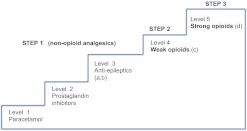
Escalation of analgesics (ie, change to a higher level of analgesic potency, classified across five levels) in association with urbanisation (five levels) and dichotomous neighbourhood deprivation was analysed over a 6-month observation period.
Ordered logistic multivariate model evaluating analgesic treatment.
In both Starter and Continuation groups, escalation was positively associated with urbanisation in a dose-response fashion (Starter group: OR (urbanisation level 1 compared with level 5): 1.24, 95% CI 1.18 to 1.30; Continuation group: OR 1.18, 95% CI 1.14 to 1.23). An additional association was apparent with neighbourhood deprivation (Starter group: OR 1.07, 95% CI 1.02 to 1.11; Continuation group: OR 1.04, 95% CI 1.01 to 1.08). Use of somatic and particularly psychotropic co-medication was associated with escalation in both groups.
Escalation of chronic analgesic treatment is associated with urban and deprived environments and occurs in a context of adding psychotropic medication prescriptions. These findings suggest that pain outcomes and mental health outcomes share factors that increase risk and remedy suffering.
鉴于城市环境与不良心理健康之间的关联,研究城市化和邻里贫困是否与慢性药物疼痛治疗中镇痛药升级有关,以及升级是否与精神药物处方有关。
对荷兰基于人群的常规配药数据库进行纵向分析。
具有代表性的药房样本,涵盖荷兰全国基层医疗和医院门诊环境中73%的药物消费。
纳入449410名15 - 85岁的患者,其中166374名属于慢性镇痛治疗的起始组,283036名属于延续组。
在6个月的观察期内,分析镇痛药升级(即改为更高效力水平的镇痛药,分为五个级别)与城市化(五个级别)和二分法邻里贫困之间的关联。
采用有序逻辑多元模型评估镇痛治疗。
在起始组和延续组中,表示升级与城市化呈剂量反应关系(起始组:城市化水平1与水平5相比的比值比(OR):1.24,95%置信区间(CI)1.18至1.30;延续组:OR 1.18,95% CI 1.14至1.23)。邻里贫困也存在额外关联(起始组:OR 1.07,95% CI 1.02至1.1;延续组:OR 1.04,95% CI 1.01至1.08)。两组中使用躯体药物尤其是精神药物联合用药与升级有关。
慢性镇痛治疗升级与城市和贫困环境有关,且发生在增加精神药物处方的背景下。这些发现表明,疼痛结局和心理健康结局存在共同的增加风险和缓解痛苦的因素。