Dept. of Ophthalmology, University Medical Center Groningen, University of Groningen, Groningen, The Netherlands.
PLoS One. 2012;7(7):e41211. doi: 10.1371/journal.pone.0041211. Epub 2012 Jul 27.
Visual field testing is an essential part of glaucoma care. It is hampered by variability related to the disease itself, response errors and fatigue. In glaucoma, blind parts of the visual field contribute to the diagnosis but--once established--not to progression detection; they only increase testing time. The aims of this study were to describe the persistence and spatial distribution of blind test locations in standard automated perimetry in glaucoma and to explore how the omission of presumed blind test locations would affect progression detection.
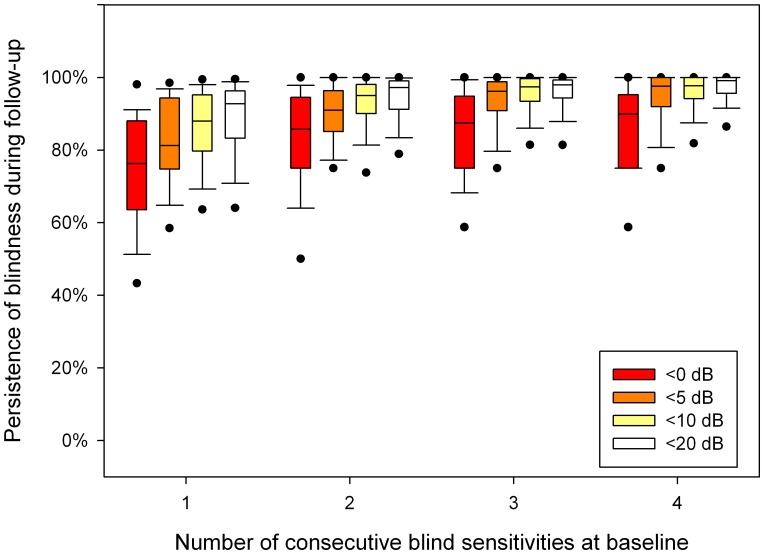
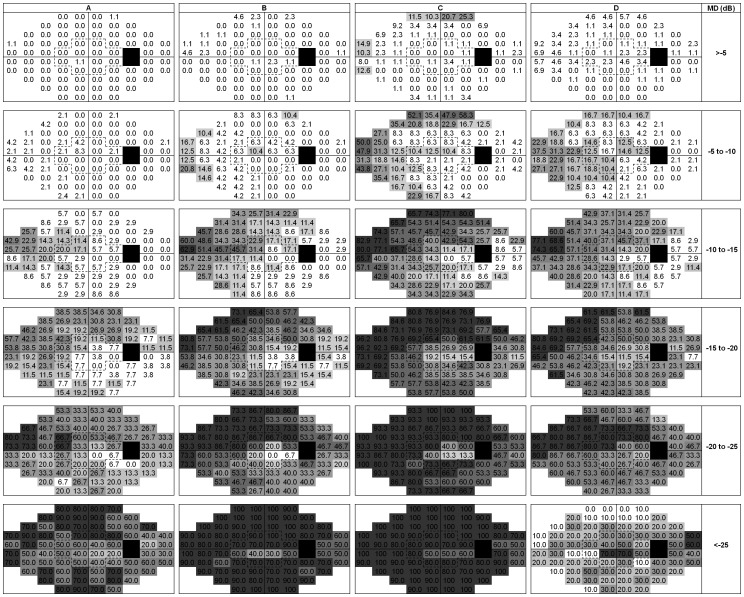
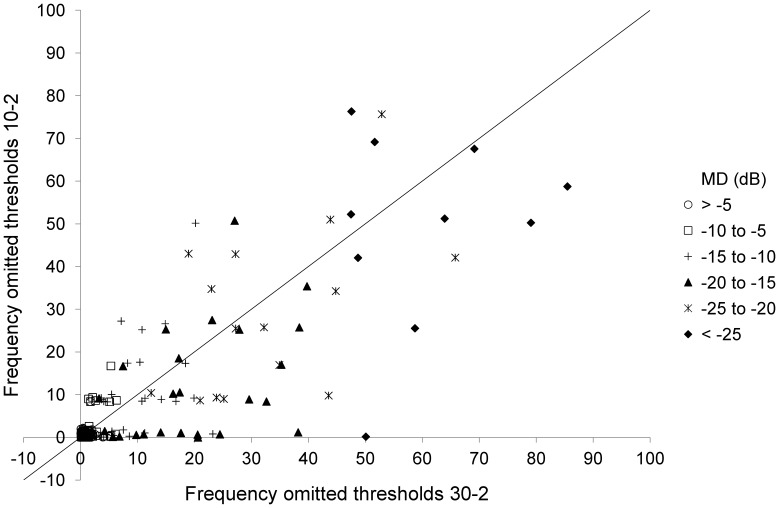
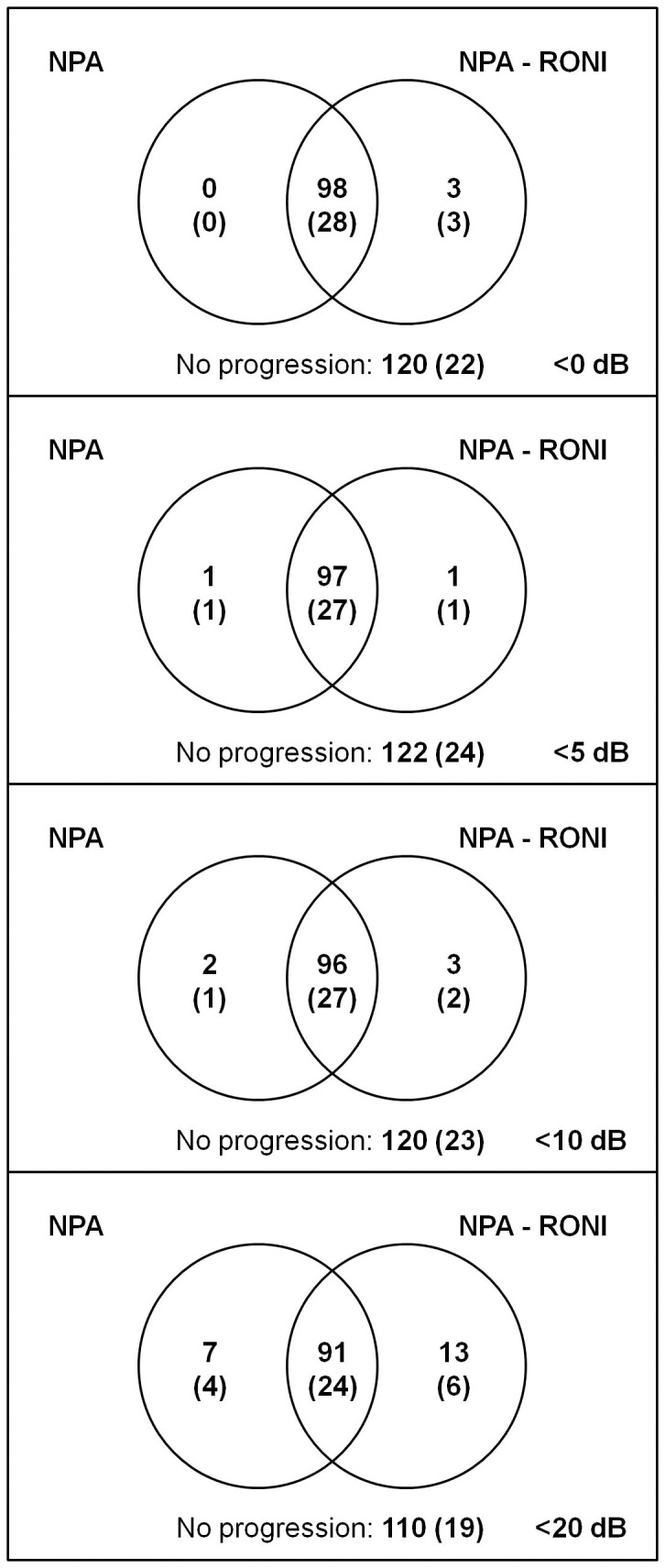
METHODOLOGY/PRINCIPAL FINDINGS: Data from 221 eyes of 221 patients from a cohort study with the Humphrey Field Analyzer with 30-2 grid were used. Patients were stratified according to baseline mean deviation (MD) in six strata of 5 dB width each. For one, two, three and four consecutive <0 dB sensitivities in the same test location in a series of baseline tests, the median probabilities to observe <0 dB again in the concerning test location in a follow-up test were 76, 86, 88 and 90%, respectively. For <10 dB, the probabilities were 88, 95, 97 and 98%, respectively. Median (interquartile range) percentages of test locations with three consecutive <0 dB sensitivities were 0(0-0), 0(0-2), 4(0-9), 17(8-27), 27(20-40) and 60(50-70)% for the six MD strata. Similar percentages were found for a subset of test locations within 10 degree eccentricity (P>0.1 for all strata). Omitting test locations with three consecutive <0 dB sensitivities at baseline did not affect the performance of the MD-based Nonparametric Progression Analysis progression detection algorithm.
CONCLUSIONS/SIGNIFICANCE: Test locations that have been shown to be reproducibly blind tend to display a reasonable blindness persistence and do no longer contribute to progression detection. There is no clinically useful universal MD cut-off value beyond which testing can be limited to 10 degree eccentricity.
视野测试是青光眼护理的重要组成部分。它受到与疾病本身、反应误差和疲劳相关的可变性的阻碍。在青光眼患者中,视野的失明部分有助于诊断,但一旦确定,就无法检测进展;它们只会增加测试时间。本研究的目的是描述标准自动视野计中青光眼的盲测位置的持久性和空间分布,并探讨忽略假定的盲测位置如何影响进展检测。
方法/主要发现:使用来自一项具有 30-2 网格的 Humphrey 视野分析仪的队列研究的 221 名患者的 221 只眼的数据。根据基线平均偏差 (MD) 将患者分为六个 5dB 宽度的分层。在同一测试位置连续出现三次<0dB 的敏感性的情况下,在后续测试中再次观察到<0dB 的测试位置的中位数概率分别为 76%、86%、88%和 90%。对于<10dB,概率分别为 88%、95%、97%和 98%。三次连续出现<0dB 敏感性的测试位置的中位数(四分位间距)百分比分别为 0(0-0)、0(0-2)、4(0-9)、17(8-27)、27(20-40)和 60(50-70)%,适用于六个 MD 分层。在 10 度偏心率内的一个测试位置子集也发现了类似的百分比(所有分层的 P>0.1)。在基线时忽略具有三个连续<0dB 敏感性的测试位置不会影响基于 MD 的非参数进展分析进展检测算法的性能。
结论/意义:已经证明可重复出现的盲测位置往往具有合理的失明持久性,不再有助于进展检测。没有临床上有用的普遍 MD 截止值可以将测试限制在 10 度偏心率内。