The Department of Radiation Oncology, University of Michigan Medical Center, Ann Arbor, MI, USA.
Radiat Oncol. 2012 Aug 1;7:127. doi: 10.1186/1748-717X-7-127.
To evaluate the influence of the maximum involvement of biopsy core (MIBC) on outcome for prostate cancer patients treated with dose-escalated external beam radiotherapy (EBRT).
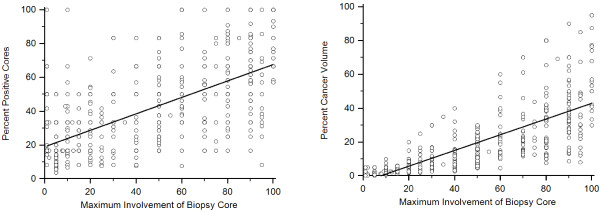
The outcomes of 590 men with localized prostate cancer treated with EBRT (≥75 Gy) at a single institution were retrospectively analyzed. The influence of MIBC on freedom from biochemical failure (FFBF), freedom from metastasis (FFM), cause-specific survival (CSS), and overall survival (OS) was compared to other surrogates for biopsy tumor volume, including the percentage of positive biopsy cores (PPC) and the total percentage of cancer volume (PCV).
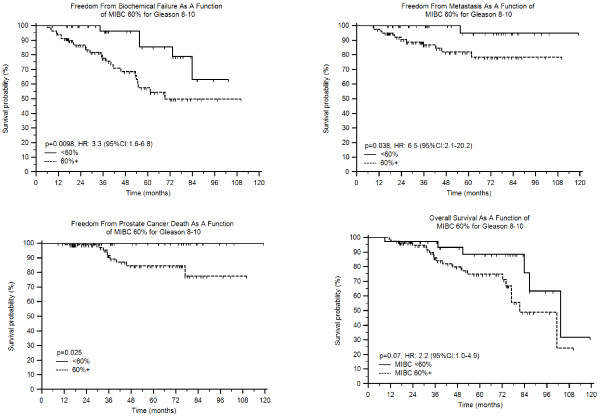
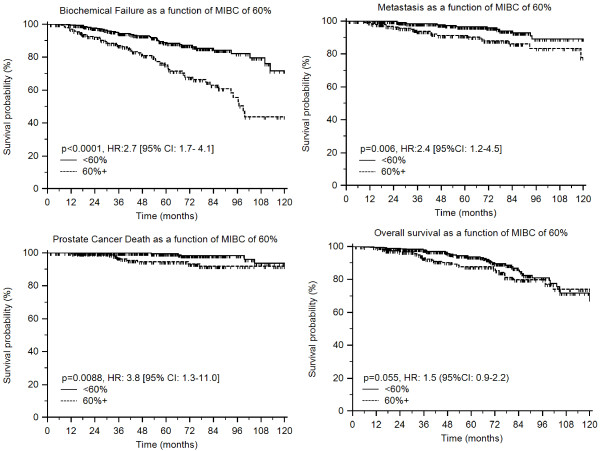
MIBC correlated with PSA, T-stage, Gleason score, NCCN risk group, PPC, PCV, and treatment related factors. On univariate analysis, MIBC was prognostic for all endpoints except OS; with greatest impact in those with Gleason scores of 8-10. However, on multivariate analysis, MIBC was only prognostic for FFBF (hazard ratio [HR] 1.9, p = 0.008), but not for FFM (p = 0.19), CSS (p = 0.16), and OS (p = 0.99).
In patients undergoing dose-escalated EBRT, MIBC had the greatest influence in those with Gleason scores of 8-10 but provided no additional prognostic data as compared to PPC and PCV, which remain the preferable prognostic variables in this patient population.
评估最大活检核心参与度(MIBC)对接受剂量递增外照射放疗(EBRT)治疗的前列腺癌患者结局的影响。
回顾性分析了 590 名在单机构接受 EBRT(≥75Gy)治疗的局限性前列腺癌患者的结局。将 MIBC 对生化无失败(FFBF)、无转移(FFM)、肿瘤特异性生存(CSS)和总生存(OS)的影响与其他活检肿瘤体积替代物(包括阳性活检核心百分比(PPC)和总癌症体积百分比(PCV))进行比较。
MIBC 与 PSA、T 分期、Gleason 评分、NCCN 风险组、PPC、PCV 和治疗相关因素相关。在单因素分析中,MIBC 对所有终点均具有预后意义,除 OS 外;在 Gleason 评分为 8-10 的患者中影响最大。然而,在多因素分析中,MIBC 仅对 FFBF 具有预后意义(风险比[HR]1.9,p=0.008),但对 FFM(p=0.19)、CSS(p=0.16)和 OS(p=0.99)无预后意义。
在接受剂量递增 EBRT 的患者中,MIBC 在 Gleason 评分为 8-10 的患者中影响最大,但与 PPC 和 PCV 相比,MIBC 并未提供额外的预后数据,PPC 和 PCV 仍然是该患者人群中首选的预后变量。