Department of Medical Physics in Radiation Oncology, DKFZ INF 280, Heidelberg, Germany.
Radiat Oncol. 2012 Aug 8;7:133. doi: 10.1186/1748-717X-7-133.
To evaluate the impact of image-guided radiation therapy (IGRT) versus non-image-guided radiation therapy (non-IGRT) on the dose to the clinical target volume (CTV) and the cervical spinal cord during fractionated intensity-modulated radiation therapy (IMRT) for head-and-neck cancer (HNC) patients.
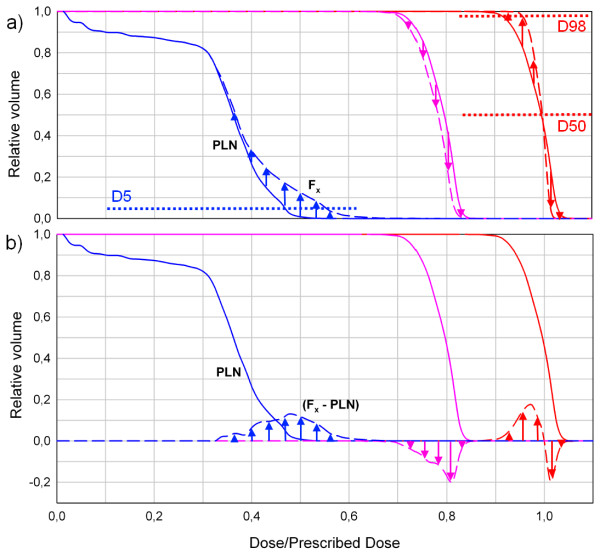
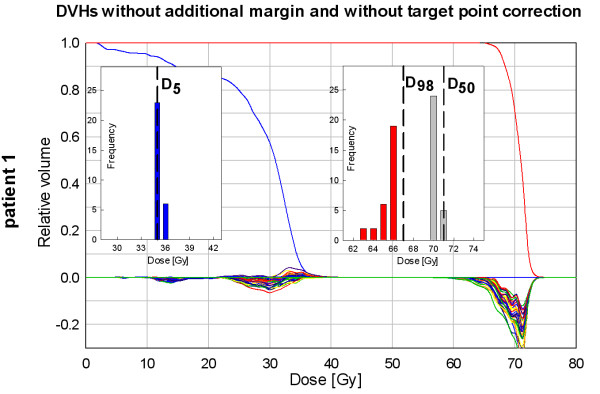
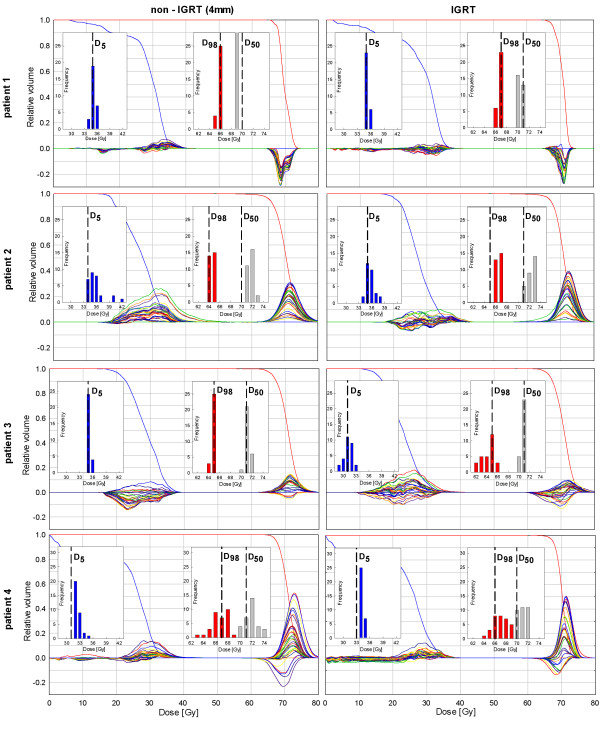
For detailed investigation, 4 exemplary patients with daily control-CT scans (total 118 CT scans) were analyzed. For the IGRT approach a target point correction (TPC) derived from a rigid registration focused to the high-dose region was used. In the non-IGRT setting, instead of a TPC, an additional cohort-based safety margin was applied. The dose distributions of the CTV and spinal cord were calculated on each control-CT and the resulting dose volume histograms (DVHs) were compared with the planned ones fraction by fraction. The D50 and D98 values for the CTV and the D5 values of the spinal cord were additionally reported.
In general, the D50 and D98 histograms show no remarkable difference between both strategies. Yet, our detailed analysis also reveals differences in individual dose coverage worth inspection. Using IGRT, the D5 histograms show that the spinal cord less frequently receives a higher dose than planned compared to the non-IGRT setting. This effect is even more pronounced when looking at the curve progressions of the respective DVHs.
Both approaches are equally effective in maintaining CTV coverage. However, IGRT is beneficial in spinal cord sparing. The use of an additional margin in the non-IGRT approach frequently results in a higher dose to the spinal cord than originally planned. This implies that a margin reduction combined with an IGRT correction helps to maintain spinal cord dose sparing best as possible. Yet, a detailed analysis of the dosimetric consequences dependent on the used strategy is required, to detect single fractions with unacceptable dosimetric deviations.
为了评估图像引导放疗(IGRT)与非图像引导放疗(non-IGRT)对头颈部癌症(HNC)患者分次调强放疗(IMRT)过程中对临床靶区(CTV)和颈脊髓剂量的影响。
详细研究了 4 例每日进行 CT 扫描的患者(共 118 次 CT 扫描)。对于 IGRT 方法,使用源自高剂量区域刚性配准的靶区点校正(TPC)。在非 IGRT 情况下,代替 TPC,应用了额外的基于 cohort 的安全余量。在每个对照 CT 上计算 CTV 和脊髓的剂量分布,并逐次比较得到的剂量体积直方图(DVH)与计划的剂量体积直方图。此外,还报告了 CTV 的 D50 和 D98 值以及脊髓的 D5 值。
一般来说,两种策略的 D50 和 D98 直方图没有明显差异。然而,我们的详细分析还揭示了值得检查的个别剂量覆盖差异。使用 IGRT,与非 IGRT 相比,脊髓接受的剂量通常低于计划剂量的 D5 直方图更频繁。当观察各自 DVH 的曲线进展时,这种效果更加明显。
两种方法在维持 CTV 覆盖方面同样有效。然而,IGRT 有利于脊髓保护。在非 IGRT 方法中使用额外的余量通常会导致脊髓接受的剂量高于最初计划的剂量。这意味着结合 IGRT 校正减少余量有助于尽可能好地维持脊髓剂量保护。然而,需要依赖于所使用的策略进行详细的剂量学后果分析,以检测具有不可接受剂量学偏差的单个分数。