Division of Preventive Medicine and Health Services Research, Institute of Population Health Sciences, National Health Research Institutes, Zhunan, Miaoli, Taiwan.
Diabetes Care. 2012 Nov;35(11):2286-92. doi: 10.2337/dc11-2052. Epub 2012 Aug 21.
The discrepancy of diabetes incidence and care between socioeconomic statuses has seldom been studied concurrently in nations with universal health coverage. We aimed to delineate whether income disparity is associated with diabetes incidence and inequality of care under a national health insurance (NHI) program in Asia.
From the Taiwan NHI database in 2000, a representative cohort aged ≥20 years and free of diabetes (n = 600,662) were followed up until 2005. We regarded individuals exempt from paying the NHI premium as being poor. Adjusted hazard ratios (HRs) were used to discover any excess risk of diabetes in the poor population. The indicators used to evaluate quality of diabetes care included the proportion of diabetic patients identified through hospitalization, visits to diabetes clinics, and completion of recommended diabetes tests.
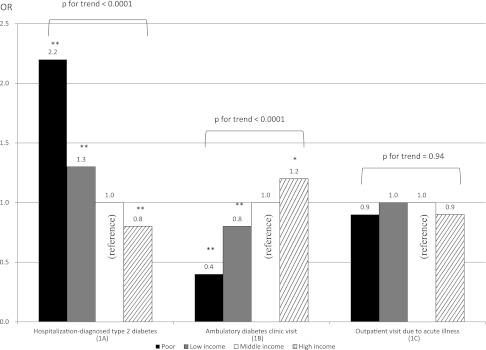
The incidence of type 2 diabetes in the poor population was 20.4 per 1,000 person-years (HR, 1.5; 95% CI, 1.3-1.7). Compared with their middle-income counterparts, the adjusted odds ratio (OR) for the poor population incidentally identified as having diabetes through hospitalization was 2.2 (P < 0.001). Poor persons with diabetes were less likely to visit any diabetes clinic (OR, 0.4; P < 0.001). The ORs for the poor population with diabetes to receive tests for glycated hemoglobin, low-density lipoprotein cholesterol, triglycerides, and retinopathy were 0.6 (0.4-0.9), 0.4 (0.2-0.7), 0.5 (0.4-0.8), and 0.4 (0.2-0.9), respectively.
Poverty is associated not only with higher diabetes incidence but also with inequality of diabetes care in a northeast Asian population, despite universal health coverage.
在全民医保覆盖的国家中,很少同时研究社会经济地位之间的糖尿病发病率和护理差异。我们旨在描述在亚洲国家的全民健康保险(NHI)计划下,收入差距是否与糖尿病发病率和护理不平等相关。
从 2000 年台湾 NHI 数据库中,我们选择了一个年龄≥20 岁且无糖尿病(n=600662)的代表性队列进行随访,直至 2005 年。我们将无需支付 NHI 保费的个人视为贫困人口。使用调整后的危险比(HR)来发现贫困人口患糖尿病的风险是否过高。评估糖尿病护理质量的指标包括通过住院、糖尿病诊所就诊和完成推荐的糖尿病检查来确定糖尿病患者的比例。
贫困人口的 2 型糖尿病发病率为 20.4/1000 人年(HR,1.5;95%CI,1.3-1.7)。与中等收入人群相比,通过住院偶然发现患有糖尿病的贫困人口的调整比值比(OR)为 2.2(P<0.001)。患有糖尿病的贫困人口就诊于任何糖尿病诊所的可能性较小(OR,0.4;P<0.001)。患有糖尿病的贫困人口接受糖化血红蛋白、低密度脂蛋白胆固醇、甘油三酯和视网膜病变检查的 OR 分别为 0.6(0.4-0.9)、0.4(0.2-0.7)、0.5(0.4-0.8)和 0.4(0.2-0.9)。
尽管全民医保覆盖,但在东北亚人群中,贫困不仅与更高的糖尿病发病率相关,而且与糖尿病护理不平等相关。