Division of Weight Management and Wellness, Children's Hospital of Pittsburgh, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania, USA.
Diabetes Care. 2012 Dec;35(12):2559-63. doi: 10.2337/dc12-0747. Epub 2012 Aug 21.
The recommended HbA(1c) diagnostic categories remain controversial and their utility in doubt in pediatrics. We hypothesized that alterations in the pathophysiologic mechanisms of type 2 diabetes may be evident in the American Diabetes Association recommended at-risk/prediabetes category (HbA(1c) 5.7 to <6.5%).
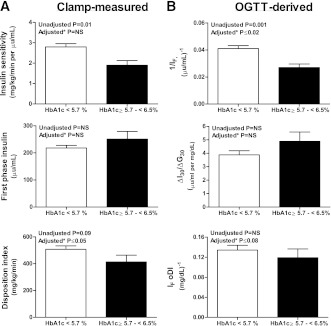
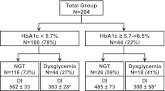
We compared in vivo hepatic and peripheral insulin sensitivity by [6,6-(2)H(2)] glucose and a 3-h hyperinsulinemic-euglycemic clamp and β-cell function by a 2-h hyperglycemic clamp (∼225 mg/dL) in overweight/obese (BMI ≥85th percentile) adolescents with prediabetes (HbA(1c) 5.7 to <6.5%) (n = 160) to those with normal HbA(1c) (<5.7%) (n = 44). β-Cell function was expressed relative to insulin sensitivity (i.e., the disposition index = insulin sensitivity × first-phase insulin).
In the prediabetes versus normal HbA(1c) category, fasting glucose, insulin, and oral glucose tolerance test (OGTT) area under the curve for glucose and insulin were significantly higher; hepatic and peripheral insulin sensitivity were lower; and β-cell function relative to insulin sensitivity was lower (366 ± 48 vs. 524 ± 25 mg/kg/min; P = 0.005). A total of 27% of youth in the normal HbA(1c) category and 41% in the prediabetes HbA(1c) category had dysglycemia (impaired fasting glucose and/or impaired glucose tolerance) by a 2-h OGTT.
Overweight/obese adolescents with HbA(1c) in the at-risk/prediabetes category demonstrate impaired β-cell function relative to insulin sensitivity, a metabolic marker for heightened risk of type 2 diabetes. Thus, HbA(1c) may be a suitable screening tool in large-scale epidemiological observational and/or interventional studies examining the progression or reversal of type 2 diabetes risk.
推荐的 HbA(1c) 诊断类别仍然存在争议,其在儿科中的应用也存在疑问。我们假设 2 型糖尿病病理生理机制的改变可能在 美国糖尿病协会推荐的高危/糖尿病前期类别(HbA(1c)5.7 至<6.5%)中显现出来。
我们比较了超重/肥胖(BMI≥85 百分位)青少年中患有糖尿病前期(HbA(1c)5.7 至<6.5%)(n=160)和 HbA(1c)正常(<5.7%)(n=44)的个体的体内肝胰岛素敏感性和外周胰岛素敏感性(通过[6,6-(2)H(2)]葡萄糖和 3 小时高胰岛素正常血糖钳夹试验评估)和β细胞功能(通过 2 小时高血糖钳夹试验(约 225mg/dL)评估)。β细胞功能相对于胰岛素敏感性进行表达(即,处置指数=胰岛素敏感性×第一相胰岛素)。
在糖尿病前期与 HbA(1c)正常组相比,空腹血糖、胰岛素和口服葡萄糖耐量试验(OGTT)的血糖和胰岛素曲线下面积均显著升高;肝胰岛素敏感性和外周胰岛素敏感性均降低;β细胞功能相对于胰岛素敏感性也降低(366±48 vs. 524±25mg/kg/min;P=0.005)。在 HbA(1c)正常组中,有 27%的青少年和在糖尿病前期 HbA(1c)组中有 41%的青少年出现了糖代谢异常(空腹血糖受损和/或糖耐量受损),通过 2 小时 OGTT 进行评估。
HbA(1c)处于高危/糖尿病前期类别的超重/肥胖青少年表现出β细胞功能相对于胰岛素敏感性受损,这是 2 型糖尿病风险增加的代谢标志物。因此,HbA(1c)可能是在大规模的流行病学观察性和/或干预性研究中筛查 2 型糖尿病风险的合适工具。