Sánchez-Quintana Damián, López-Mínguez José Ramón, Pizarro Gonzalo, Murillo Margarita, Cabrera José Angel
Departamento de Anatomía y Biología Celular, Facultad de Medicina, Universidad de Extremadura, Badajoz, Spain.
Curr Cardiol Rev. 2012 Nov;8(4):310-26. doi: 10.2174/157340312803760721.
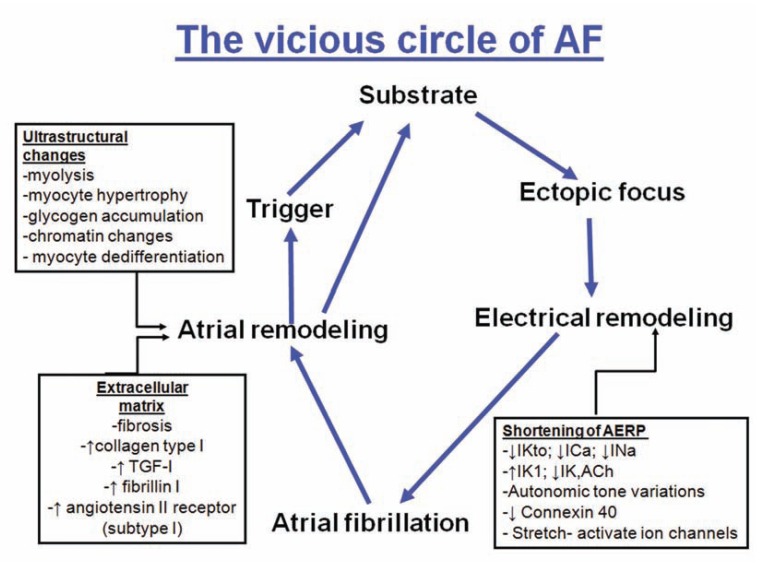
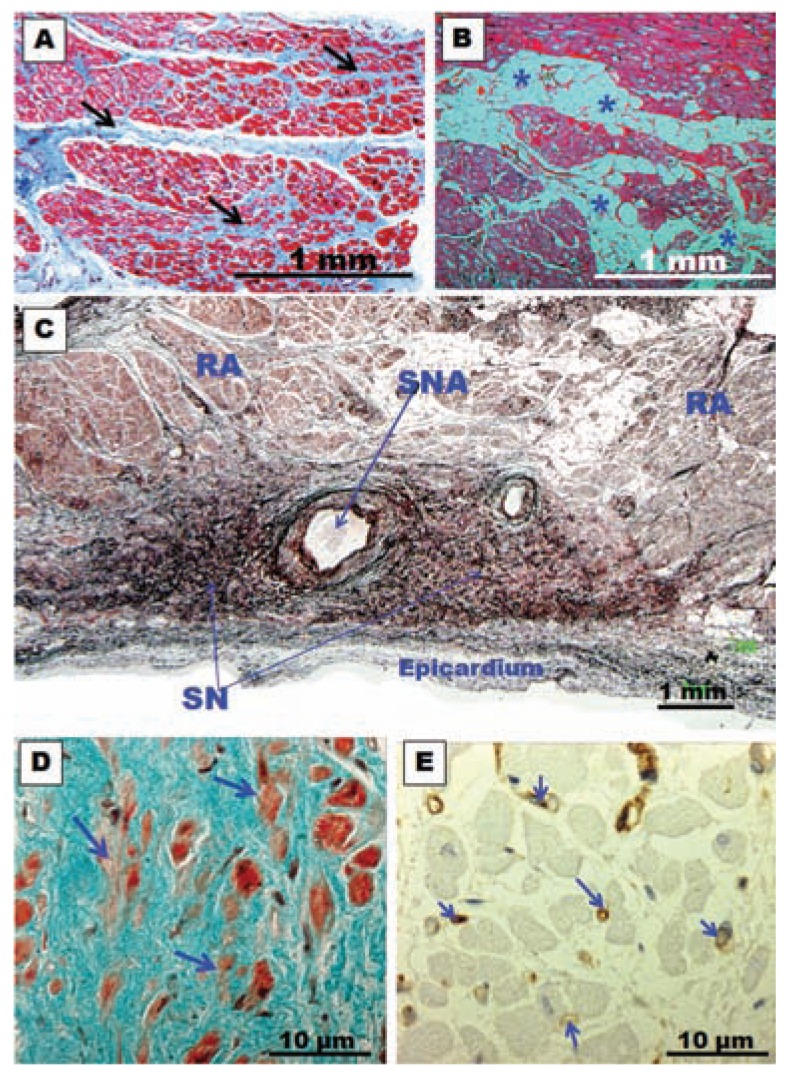
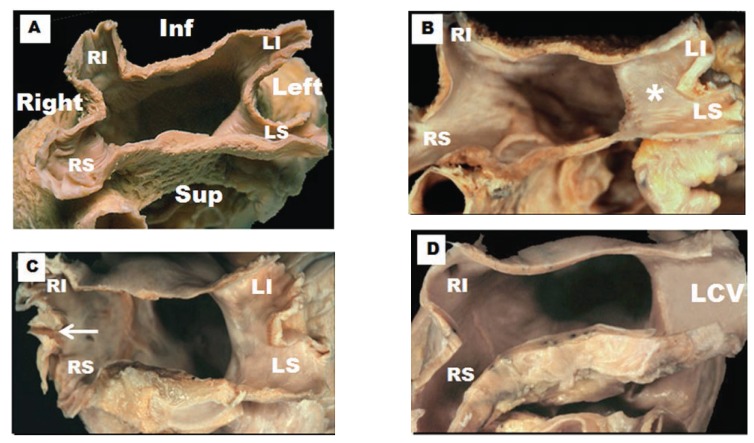
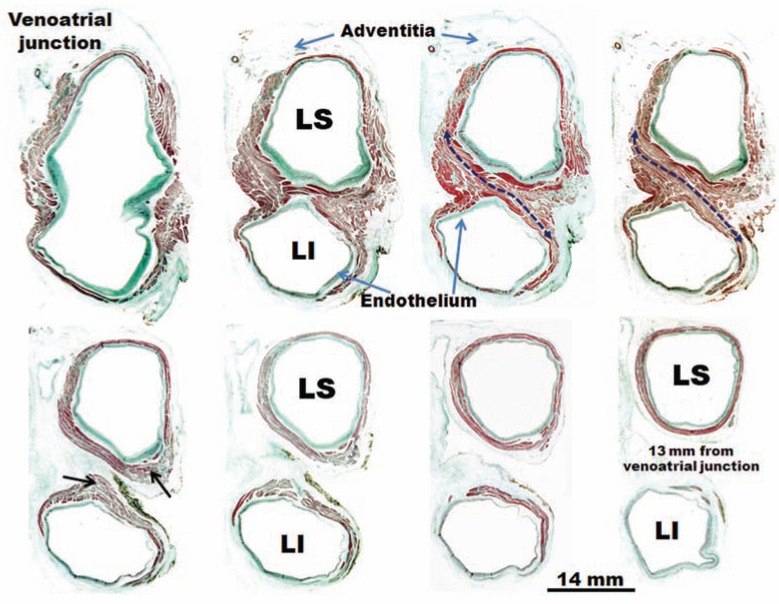
The definition of atrial fibrillation (AF) as a functional electrical disorder does not reflect the significant underlying structural abnormalities. Atrial and Pulmonary Vein (PV) muscle sleeve microstructural remodeling is present, and establishes a vulnerable substrate for AF maintenance. In spite of an incomplete understanding of the anatomo-functional basis for AF, current evidence demonstrates that this arrhythmia usually requires a trigger for initiation and a vulnerable electrophysiological and/or anatomical substrate for maintenance. It is still unclear whether the trigger mechanisms include focal enhanced automaticity, triggered activity and/or micro re-entry from myocardial tissue. Initiation of AF can be favored by both parasympathetic and sympathetic stimulation, which also seem to play a role in maintaining AF. Finally, evolving clinical evidence demonstrates that inflammation is associated with new-onset and recurrent AF through a mechanism that possibly involves cellular degeneration, apoptosis, and subsequent atrial fibrosis.
将心房颤动(AF)定义为功能性电紊乱并不能反映其显著的潜在结构异常。心房和肺静脉(PV)肌袖存在微观结构重塑,为房颤的维持建立了一个易损基质。尽管对房颤的解剖功能基础了解不完整,但目前的证据表明,这种心律失常通常需要一个触发因素来启动,并需要一个易损的电生理和/或解剖学基质来维持。触发机制是否包括局灶性自律性增强、触发活动和/或心肌组织的微折返仍不清楚。副交感神经和交感神经刺激都可能促进房颤的启动,它们似乎也在维持房颤中发挥作用。最后,不断发展的临床证据表明,炎症通过可能涉及细胞变性、凋亡及随后心房纤维化的机制与新发和复发性房颤相关。