Duke Clinical Research Institute, Durham, NC 27705, USA.
Am J Med. 2012 Nov;125(11):1085-94. doi: 10.1016/j.amjmed.2012.04.038. Epub 2012 Aug 22.
Substantial heterogeneity in hospital length of stay exists among patients admitted with non-ST-segment elevation myocardial infarction. Furthermore, little is known about the factors that impact length of stay.
We examined 39,107 non-ST-segment elevation myocardial infarction patients admitted to 351 Acute Coronary Treatment Intervention Outcomes Network Registry-Get With The Guidelines hospitals from January 1, 2007-March 31, 2009 who underwent cardiac catheterization and survived to discharge. Length of stay was categorized into 4 groups (≤2, 3-4, 5-7, and ≥8 days), where prolonged length of stay was defined as >4 days.
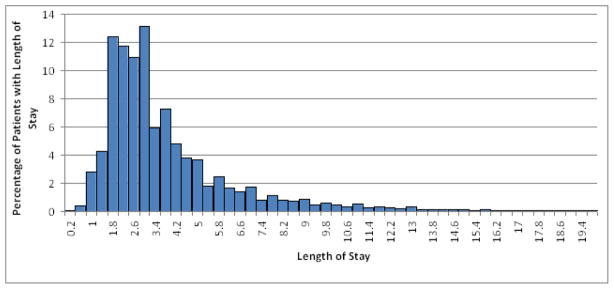
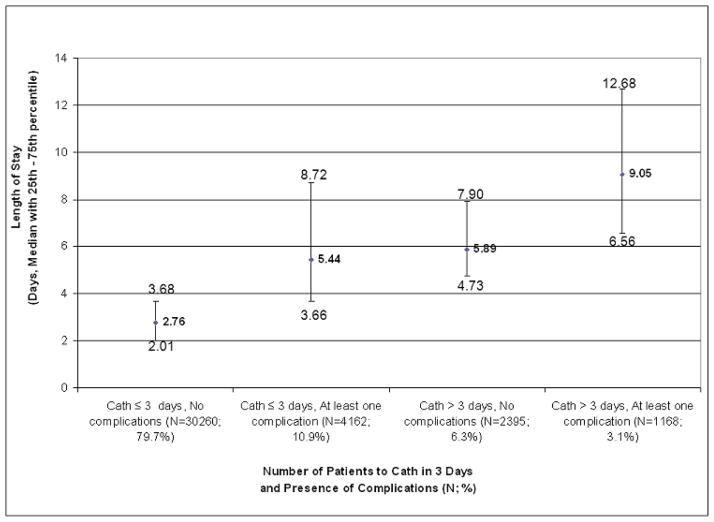
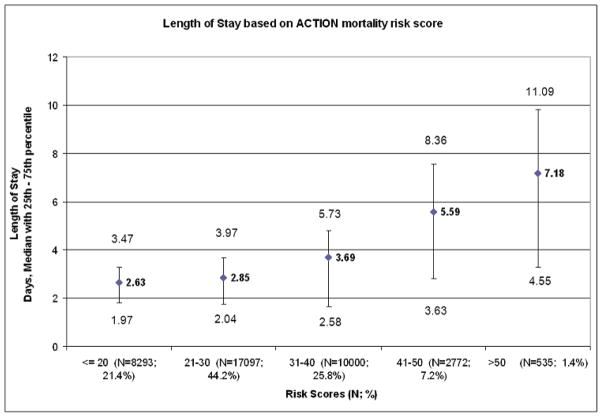
The overall median (25(th), 75(th)) length of stay was 3 (2, 5) days. Patients with a length of stay of >2 days were older with more comorbidities, but were less likely to receive evidence-based therapies or percutaneous coronary intervention. Among the factors associated with prolonged length of stay >4 days were delay to cardiac catheterization >48 hours, heart failure or shock on admission, female sex, insurance type, and admission to the hospital on a Friday afternoon or evening. Hospital characteristics such as academic versus nonacademic or urban versus rural setting, were not associated with prolonged length of stay.
Patients with longer length of stay have more comorbidities and in-hospital complications, yet paradoxically, are less often treated with evidence-based medications and are less likely to receive percutaneous coronary intervention. Hospital admission on a Friday afternoon or evening and delays to catheterization appear to significantly impact length of stay. A better understanding of factors associated with length of stay in patients with non-ST-segment elevation myocardial infarction is needed to promote safe and early discharge in an era of increasingly restrictive health care resources.
非 ST 段抬高型心肌梗死患者的住院时间存在很大差异。此外,影响住院时间的因素知之甚少。
我们研究了 2007 年 1 月 1 日至 2009 年 3 月 31 日期间在 351 家急性冠状动脉治疗干预结果网络注册-遵循指南(Acute Coronary Treatment Intervention Outcomes Network Registry-Get With The Guidelines,ACTION)注册的 39107 名接受过心脏导管检查且存活至出院的非 ST 段抬高型心肌梗死患者。住院时间分为 4 组(≤2、3-4、5-7 和≥8 天),其中延长住院时间定义为>4 天。
总体中位数(25%,75%)住院时间为 3(2,5)天。住院时间>2 天的患者年龄较大,合并症更多,但接受循证治疗或经皮冠状动脉介入治疗的可能性较小。与>4 天的住院时间延长相关的因素包括心脏导管检查延迟>48 小时、入院时心力衰竭或休克、女性、保险类型以及周五下午或晚上入院。与住院时间延长相关的因素还包括医院特征,如学术医院与非学术医院或城市医院与农村医院,与住院时间延长无关。
住院时间较长的患者合并症和院内并发症更多,但矛盾的是,接受循证药物治疗的可能性较小,接受经皮冠状动脉介入治疗的可能性也较小。周五下午或晚上入院以及心脏导管检查延迟似乎会显著影响住院时间。需要更好地了解非 ST 段抬高型心肌梗死患者住院时间的相关因素,以在医疗资源日益受限的时代促进安全和早期出院。