Norwich Medical School, University of East Anglia, Norwich, UK.
Trials. 2012 Aug 27;13:151. doi: 10.1186/1745-6215-13-151.
Computerised cognitive behaviour therapy (cCBT) involves standardised, automated, interactive self-help programmes delivered via a computer. Randomised controlled trials (RCTs) and observational studies have shown than cCBT reduces depressive symptoms as much as face-to-face therapy and more than waiting lists or treatment as usual. cCBT's efficacy and acceptability may be influenced by the "human" support offered as an adjunct to it, which can vary in duration and can be offered by people with different levels of training and expertise.
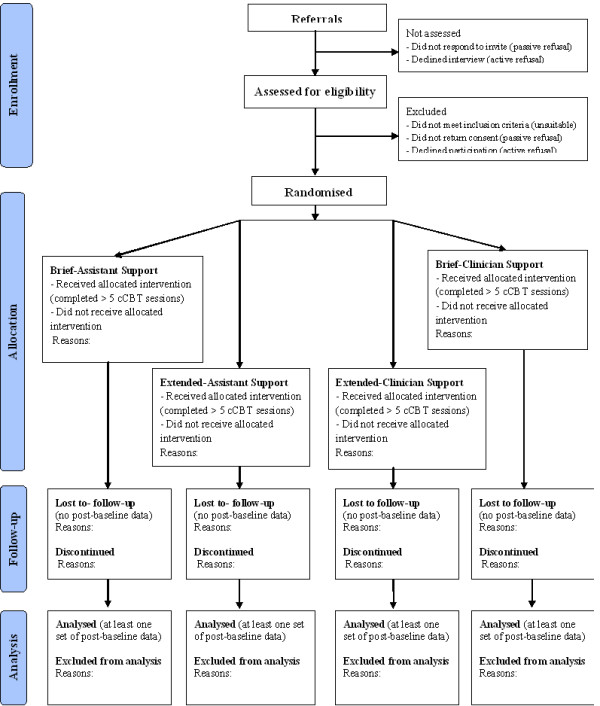
METHODS/DESIGN: This is a two-by-two factorial RCT investigating the effectiveness, cost-effectiveness and acceptability of cCBT supplemented with 12 weekly phone support sessions are either brief (5-10 min) or extended (20-30 min) and are offered by either an expert clinician or an assistant with no clinical training. Adults with non-suicidal depression in primary care can self-refer into the study by completing and posting to the research team a standardised questionnaire. Following an assessment interview, eligible referrals have access to an 8-session cCBT programme called Beating the Blues and are randomised to one of four types of support: brief-assistant, extended-assistant, brief-clinician or extended-clinician.A sample size of 35 per group (total 140) is sufficient to detect a moderate effect size with 90% power on our primary outcome measure (Work and Social Adjustment Scale); assuming a 30% attrition rate, 200 patients will be randomised. Secondary outcome measures include the Beck Depression and Anxiety Inventories and the PHQ-9 and GAD-7. Data on clinical outcomes, treatment usage and patient experiences are collected in three ways: by post via self-report questionnaires at week 0 (randomisation) and at weeks 12 and 24 post-randomisation; electronically by the cCBT system every time patients log-in; by phone during assessments, support sessions and exit interviews.
The study's factorial design increases its efficiency by allowing the concurrent investigation of two types of adjunct support for cCBT with a single sample of participants. Difficulties in recruitment, uptake and retention of participants are anticipated because of the nature of the targeted clinical problem (depression impairs motivation) and of the studied interventions (lack of face-to-face contact because referrals, assessments, interventions and data collection are completed by phone, computer or post).
Current Controlled Trials ISRCTN98677176.
计算机化认知行为疗法(cCBT)涉及通过计算机提供标准化、自动化、交互式自助计划。随机对照试验(RCT)和观察性研究表明,cCBT 可减轻抑郁症状,与面对面治疗一样有效,甚至比等待名单或常规治疗更有效。cCBT 的疗效和可接受性可能受到作为其辅助手段提供的“人为”支持的影响,这种支持在持续时间上可能有所不同,并且可以由具有不同培训和专业水平的人员提供。
方法/设计:这是一项两因素析因 RCT,旨在调查补充 12 周每周电话支持的 cCBT 的有效性、成本效益和可接受性,这些支持可以是简短的(5-10 分钟)或延长的(20-30 分钟),并且由专家临床医生或没有临床培训的助手提供。初级保健中非自杀性抑郁症患者可以通过填写并寄给研究团队一份标准化问卷,自行向研究注册。在评估面谈后,符合条件的转诊患者可以使用名为“战胜忧郁”的 8 节 cCBT 计划,并随机分配到四种支持类型之一:简短助手、延长助手、简短临床医生或延长临床医生。每组 35 人的样本量(共 140 人)足以在我们的主要结果测量(工作和社会调整量表)上以 90%的功率检测到中等效应大小;假设 30%的脱落率,将有 200 名患者被随机分配。次要结果测量包括贝克抑郁和焦虑量表以及 PHQ-9 和 GAD-7。通过以下三种方式收集临床结果、治疗使用情况和患者体验的数据:通过邮寄,在随机分组时(第 0 周)和随机分组后 12 周和 24 周时通过自我报告问卷;通过电子方式,每次患者登录时通过 cCBT 系统;通过电话,在评估、支持会议和退出访谈期间。
该研究的析因设计通过允许对 cCBT 的两种类型的辅助支持进行同时调查,提高了其效率,同时使用单一参与者样本。由于目标临床问题(抑郁会损害动机)和研究干预措施(由于转介、评估、干预和数据收集通过电话、计算机或邮寄完成,因此缺乏面对面接触)的性质,预计参与者的招募、参与和保留会遇到困难。
当前对照试验 ISRCTN98677176。