The George Institute for Global Health, The University of Sydney, Sydney, Australia.
PLoS Med. 2012;9(8):e1001293. doi: 10.1371/journal.pmed.1001293. Epub 2012 Aug 21.
Guidelines recommend intensive blood pressure (BP) lowering in patients at high risk. While placebo-controlled trials have demonstrated 22% reductions in coronary heart disease (CHD) and stroke associated with a 10-mmHg difference in systolic BP, it is unclear if more intensive BP lowering strategies are associated with greater reductions in risk of CHD and stroke. We did a systematic review to assess the effects of intensive BP lowering on vascular, eye, and renal outcomes.
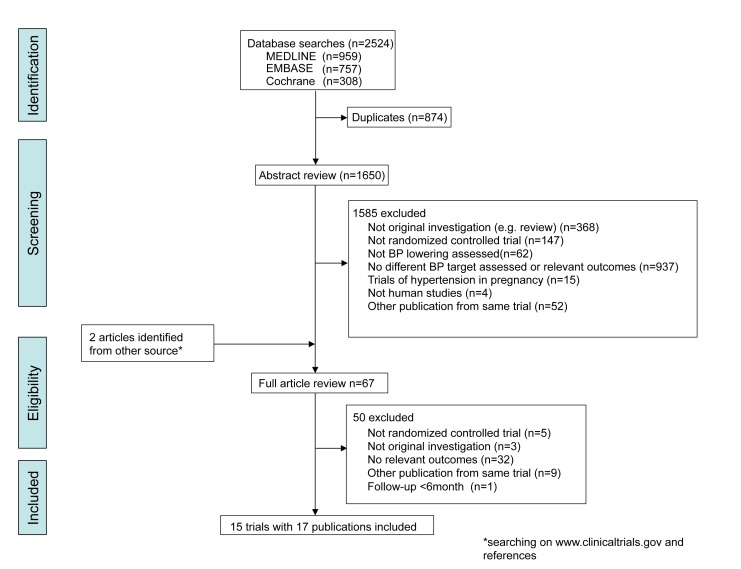
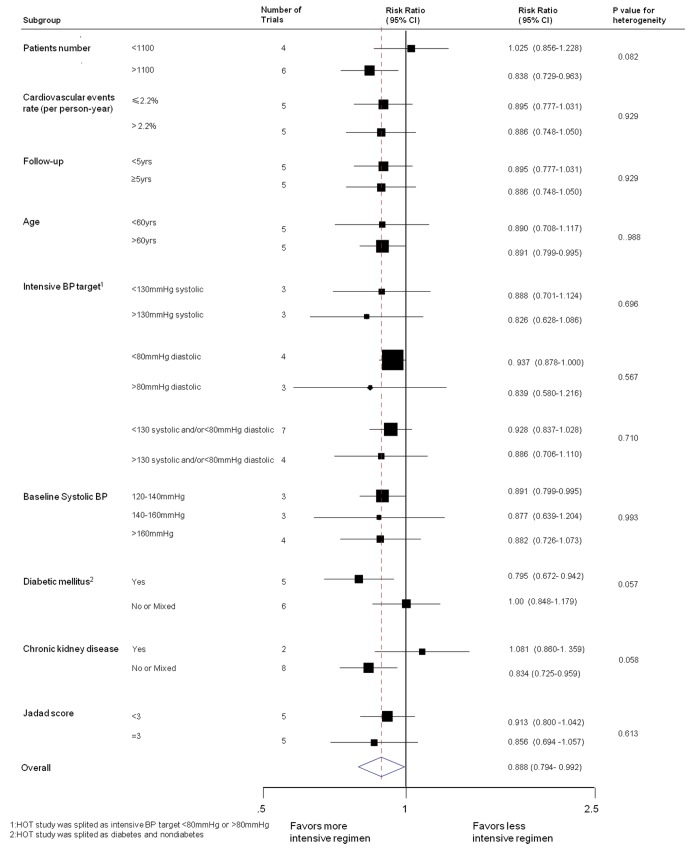
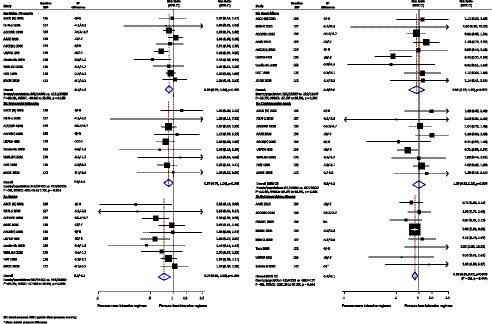
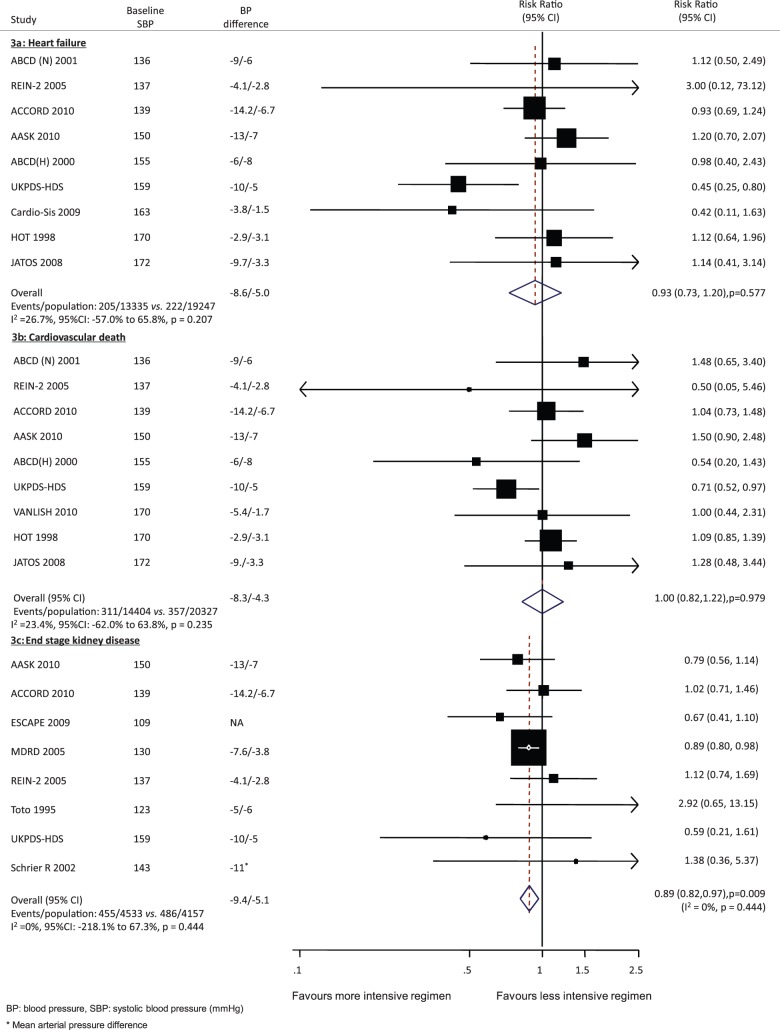
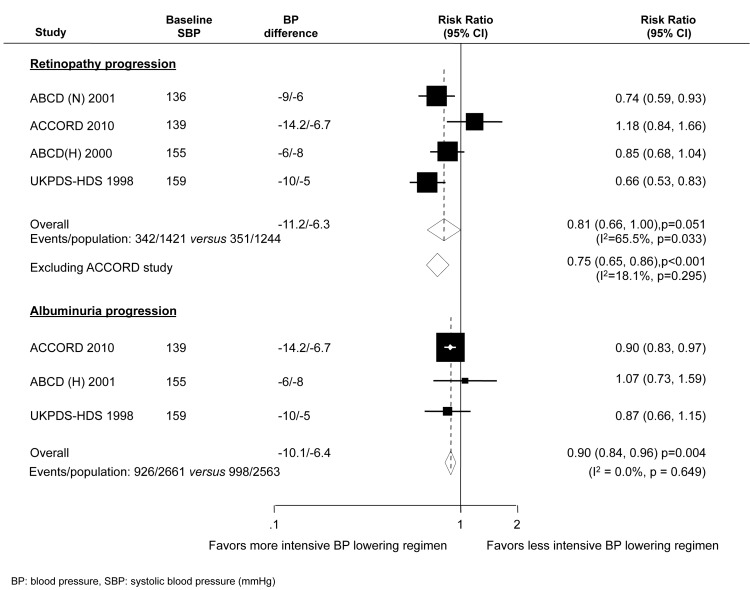
We systematically searched Medline, Embase, and the Cochrane Library for trials published between 1950 and July 2011. We included trials that randomly assigned individuals to different target BP levels. We identified 15 trials including a total of 37,348 participants. On average there was a 7.5/4.5-mmHg BP difference. Intensive BP lowering achieved relative risk (RR) reductions of 11% for major cardiovascular events (95% CI 1%-21%), 13% for myocardial infarction (0%-25%), 24% for stroke (8%-37%), and 11% for end stage kidney disease (3%-18%). Intensive BP lowering regimens also produced a 10% reduction in the risk of albuminuria (4%-16%), and a trend towards benefit for retinopathy (19%, 0%-34%, p = 0.051) in patients with diabetes. There was no clear effect on cardiovascular or noncardiovascular death. Intensive BP lowering was well tolerated; with serious adverse events uncommon and not significantly increased, except for hypotension (RR 4.16, 95% CI 2.25 to 7.70), which occurred infrequently (0.4% per 100 person-years).
Intensive BP lowering regimens provided greater vascular protection than standard regimens that was proportional to the achieved difference in systolic BP, but did not have any clear impact on the risk of death or serious adverse events. Further trials are required to more clearly define the risks and benefits of BP targets below those currently recommended, given the benefits suggested by the currently available data.
指南建议高危患者强化降压。虽然安慰剂对照试验已经证明,收缩压降低 10mmHg 可使冠心病(CHD)和中风风险降低 22%,但目前尚不清楚更强化的降压策略是否会降低 CHD 和中风的风险。我们进行了系统评价以评估强化降压对血管、眼部和肾脏结局的影响。
我们系统地检索了 Medline、Embase 和 Cochrane 图书馆中 1950 年至 2011 年 7 月发表的试验。我们纳入了将个体随机分配至不同目标血压水平的试验。我们共纳入了 15 项试验,总计 37348 名参与者。平均收缩压差异为 7.5/4.5mmHg。强化降压实现了主要心血管事件相对风险(RR)降低 11%(95% CI 1%-21%)、心肌梗死降低 13%(0%-25%)、中风降低 24%(8%-37%)、终末期肾病降低 11%(3%-18%)。强化降压方案还使蛋白尿风险降低 10%(4%-16%),糖尿病患者的视网膜病变也有获益趋势(19%,0%-34%,p=0.051)。但对心血管或非心血管死亡无明显影响。强化降压耐受良好,严重不良事件不常见且未显著增加,除低血压(RR 4.16,95% CI 2.25 至 7.70)外,低血压的发生率较低(每 100 人年 0.4%)。
与标准降压方案相比,强化降压方案可提供更大的血管保护作用,与收缩压降低的差异成正比,但对死亡或严重不良事件的风险没有任何明确影响。鉴于目前可用数据提示获益,需要进一步的试验来更明确地定义低于目前推荐靶目标的血压的风险和获益。