Section of Advanced Heart Failure and Transplantation, University of Colorado Anschutz Medical Campus, Aurora, USA.
J Med Econ. 2013;16(1):43-54. doi: 10.3111/13696998.2012.726932. Epub 2012 Sep 13.
Descriptions of the inpatient experience for patients hospitalized with systolic heart failure (HF) are limited and lack a cross-sectional representation of the US population. While length of stay (LOS) is a primary determinant of resource use and post-discharge events, few models exist for estimating LOS.
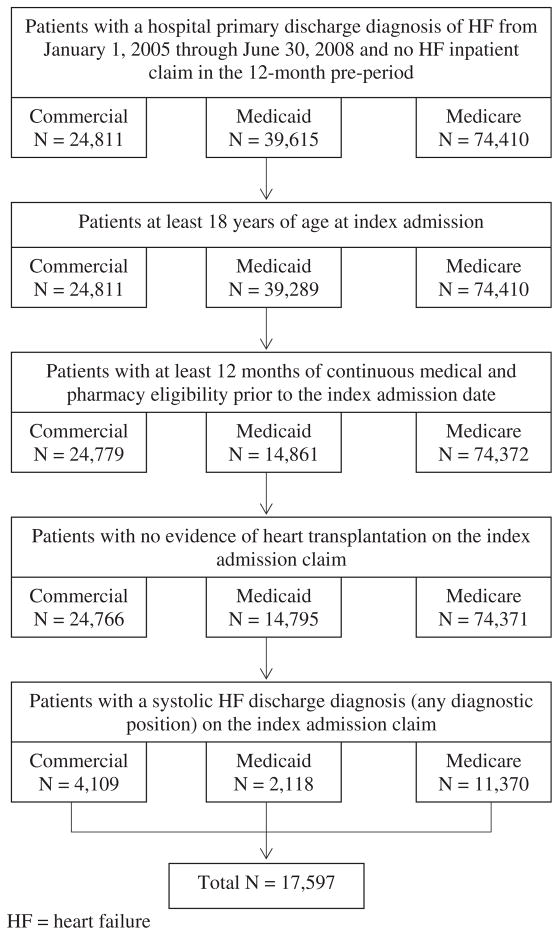
MarketScan(®) administrative claims data from 1/1/2005-6/30/2008 were used to select hospitalized patients aged ≥18 years with discharge diagnoses for both HF (primary diagnosis) and systolic HF (any diagnostic position) without prior HF hospitalization or undergoing transplantation.
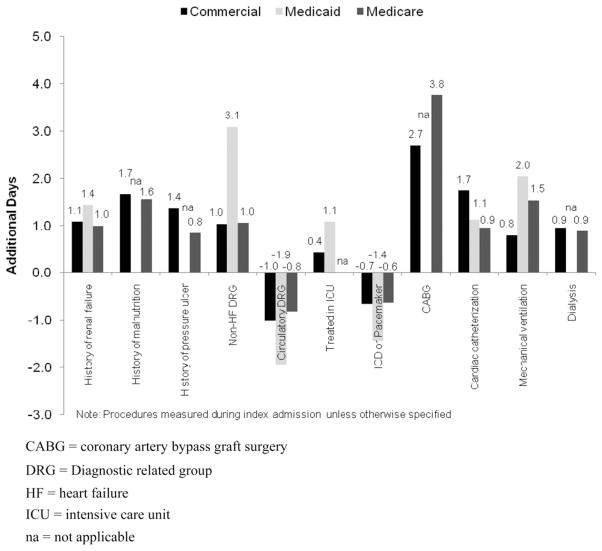
Among 17,597 patients with systolic HF; 4109 had commercial; 2118 had Medicaid; and 11,370 had Medicare payer type. Medicaid patients had longer mean LOS (7.1 days) than commercial (6.3 days) or Medicare (6.7 days). In-hospital mortality was highest for patients with Medicaid (2.4%), followed by Medicare (1.3%) and commercial (0.6%). Commercial patients were more likely to receive inpatient procedures. Renal failure, pressure ulcer, malnutrition, a non-circulatory index admission DRG, receipt of a coronary artery bypass procedure or cardiac catheterization, or need for mechanical ventilation during the index admission were associated with increased LOS; receipt of a pacemaker device at index was associated with shorter LOS.
Selection of patients with systolic HF is limited by completeness and accuracy of medical coding, and results may not be generalizable to patients with diastolic HF or to international populations.
Inpatient care, LOS, and in-hospital survival differ by payer among patients hospitalized with systolic HF, although co-morbidity and inpatient procedures consistently influence LOS across payer types. These findings may refine risk stratification, allowing for targeted intensive inpatient management and/or aggressive transitional care to improve outcomes and increase the efficiency of care.
患有收缩性心力衰竭(HF)住院患者的住院经历描述有限,且缺乏对美国人群的横断面代表性。尽管住院时间(LOS)是资源利用和出院后事件的主要决定因素,但目前很少有模型可以估计 LOS。
使用 MarketScan(®)行政索赔数据(1/1/2005-6/30/2008)选择年龄≥18 岁的住院患者,这些患者有 HF(主要诊断)和收缩性 HF(任何诊断位置)的出院诊断,无先前 HF 住院或接受移植。
在 17597 例收缩性 HF 患者中;4109 例为商业保险;2118 例为医疗补助;11370 例为医疗保险。医疗补助患者的平均 LOS(7.1 天)长于商业保险(6.3 天)或医疗保险(6.7 天)。医疗补助患者的院内死亡率最高(2.4%),其次是医疗保险(1.3%)和商业保险(0.6%)。商业保险患者更有可能接受住院治疗。入院时肾功能衰竭、压疮、营养不良、非循环指数入院 DRG、接受冠状动脉旁路手术或心导管检查、或需要机械通气与 LOS 增加相关;入院时安装起搏器与 LOS 缩短相关。
收缩性 HF 患者的选择受到医疗编码完整性和准确性的限制,结果可能不适用于舒张性 HF 患者或国际人群。
在患有收缩性 HF 的住院患者中,不同的付款人在住院治疗、LOS 和院内生存率方面存在差异,尽管合并症和住院治疗始终会影响不同付款类型的 LOS。这些发现可以完善风险分层,使针对性的强化住院管理和/或积极的过渡性护理成为可能,从而改善结局并提高护理效率。