School of Dentistry and Oral Health, Griffith University, Queensland, Australia.
BMC Infect Dis. 2012 Sep 11;12:210. doi: 10.1186/1471-2334-12-210.
Human herpesvirus 8 (HHV-8), the aetiological agent of Kaposi's sarcoma (KS), multicentric Castleman's disease (MCD), and primary effusion lymphoma (PEL) is rare in Australia, but endemic in Sub-Saharan Africa, parts of South-east Asia and Oceania. While the treatment of external KS lesions can be monitored by clinical observation, the internal lesions of KS, MCD and PEL require extensive and expensive internal imaging, or autopsy. In patients with MCD and PEL, if HHV-8 viraemia is not reduced quickly, ~50% die within 24 months. HHV-8 qPCR is a valuable tool for monitoring HHV-8 viraemia, but is not available in many parts of the world, including those with high prevalence of KS and HHV-8.
A new molecular facility with stringent three-phase workflow was established, adhering to NPAAC and CLSI guidelines. Three fully validated quantitative assays were developed: two for detection and quantification of HHV-8; one for GAPDH, necessary for normalisation of viral loads in tissue and peripheral blood.
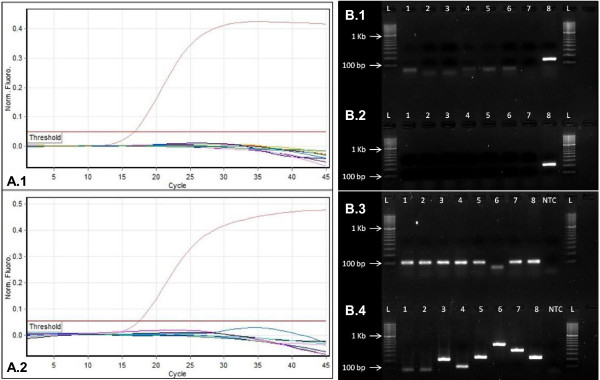
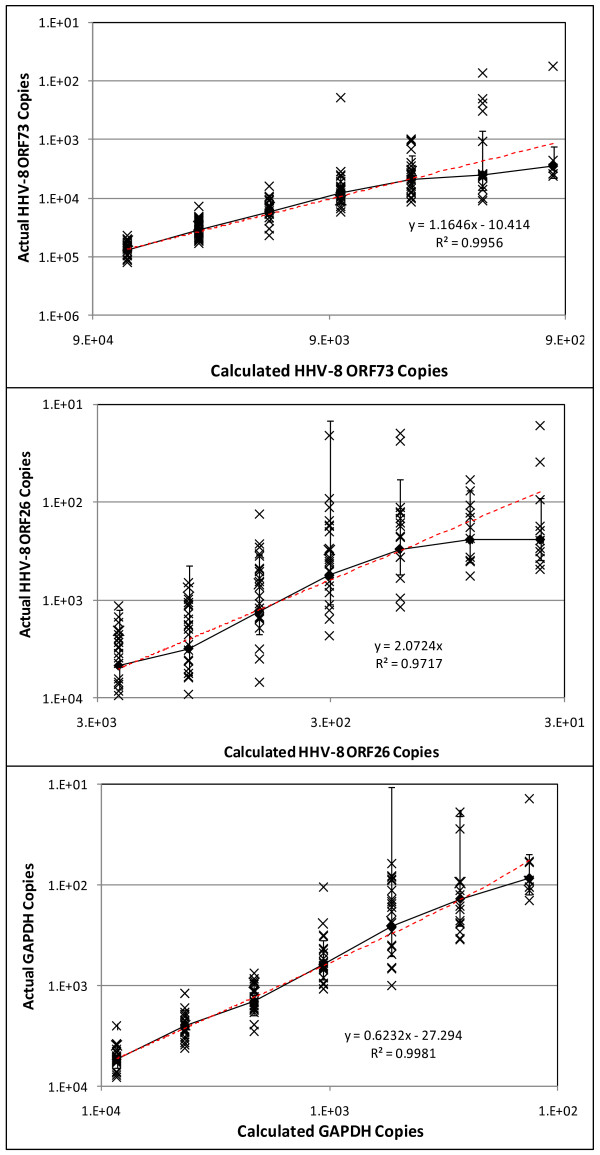
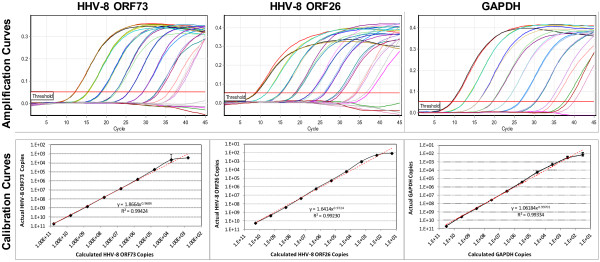
The HHV-8 ORF73 and ORF26 qPCR assays were 100% specific. All qPCR assays, displayed a broad dynamic range (102 to 1010 copies/μL TE Buffer) with a limit of detection of 4.85x103, 5.61x102, and 2.59x102 copies/μL TE Buffer and a limit of quantification of 4.85x103, 3.01x102, and 1.38x102 copies/μL TE Buffer for HHV-8 ORF73, HHV-8 ORF26, and GAPDH respectively.The assays were tested on a panel of 35 KS biopsies from Queensland. All were HHV-8 qPCR positive with average viral load of 2.96x105 HHV-8 copies/μL DNA extract (range: 4.37x103 to 1.47x106 copies/μL DNA extract): When normalised these equate to an average viral load of 2.44x104 HHV-8 copies/103 cells (range: 2.20x102 to 7.38x105 HHV-8 copies/103 cells).
These are the first fully optimised, validated and MIQE compliant HHV-8 qPCR assays established in Australia. They worked well for qualitative detection of HHV-8 in archival tissue, and are well-suited for quantitative detection in whole blood. They are now available for research, for clinical diagnosis of HHV-8 infection, and for monitoring treatment efficacy.
人类疱疹病毒 8 型(HHV-8)是卡波西肉瘤(KS)、多中心Castleman 病(MCD)和原发性渗出性淋巴瘤(PEL)的病因,在澳大利亚很少见,但在撒哈拉以南非洲、东南亚和大洋洲部分地区流行。虽然可以通过临床观察监测外部 KS 病变的治疗情况,但 KS、MCD 和 PEL 的内部病变需要广泛而昂贵的内部成像或尸检。在 MCD 和 PEL 患者中,如果 HHV-8 病毒血症不能迅速减少,约有 50%的患者在 24 个月内死亡。HHV-8 qPCR 是监测 HHV-8 病毒血症的一种有价值的工具,但在包括 KS 和 HHV-8 高发地区在内的世界许多地区都无法获得。
建立了一个具有严格三阶段工作流程的新分子设施,遵循 NPAAC 和 CLSI 指南。开发了三个完全验证的定量检测方法:两个用于检测和定量检测 HHV-8;一个用于 GAPDH,这对于组织和外周血中病毒载量的归一化是必要的。
HHV-8 ORF73 和 ORF26 qPCR 检测方法具有 100%的特异性。所有 qPCR 检测方法均显示出广泛的动态范围(102 至 1010 拷贝/μL TE 缓冲液),检测限为 4.85x103、5.61x102 和 2.59x102 拷贝/μL TE 缓冲液,定量限为 4.85x103、3.01x102 和 1.38x102 拷贝/μL TE 缓冲液,用于 HHV-8 ORF73、HHV-8 ORF26 和 GAPDH。这些检测方法在昆士兰州的 35 个 KS 活检样本中进行了测试。所有样本均为 HHV-8 qPCR 阳性,平均病毒载量为 2.96x105 HHV-8 拷贝/μL DNA 提取物(范围:4.37x103 至 1.47x106 拷贝/μL DNA 提取物):经归一化后,这些相当于平均病毒载量为 2.44x104 HHV-8 拷贝/103 个细胞(范围:2.20x102 至 7.38x105 HHV-8 拷贝/103 个细胞)。
这些是澳大利亚首次建立的完全优化、验证和 MIQE 合规的 HHV-8 qPCR 检测方法。它们在检测存档组织中的 HHV-8 定性方面表现良好,非常适合全血的定量检测。它们现在可用于研究、HHV-8 感染的临床诊断以及治疗效果的监测。