Cancer Epidemiology Unit, San Giovanni Battista Hospital, CPO Piemonte and University of Turin, Via Santena 7, 10129, Torino, Italy.
BMC Public Health. 2012 Sep 12;12:775. doi: 10.1186/1471-2458-12-775.
The present study focuses on the analysis of social, clinical and hospital characteristics that can lead to disparities in the management and outcome of care. To that end, indicators of the quality of initial treatment delivered to newly-diagnosed colorectal cancer patients in a North-Western Region of Italy, were investigated using administrative data.
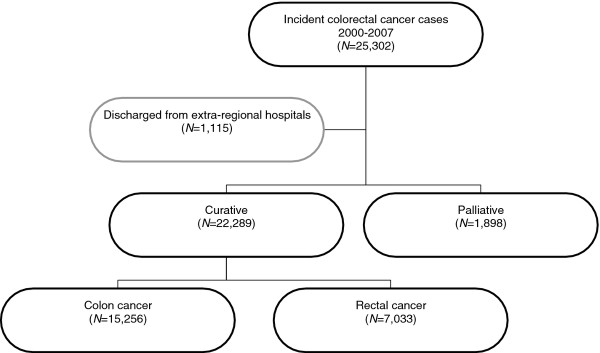
The cohort includes all incident colorectal cancer patients (N = 24,187) selected by a validated algorithm from the Piedmont Hospital Discharge Record system over an 8-year period (2000-2007).Three indicators of quality of care in this population-based cohort were evaluated: the proportion of preoperative radiotherapy (RT) and of abdominoperineal (AP) resection in rectal cancer patients, and the proportion of postoperative in-hospital mortality in colorectal cancer patients.
Among rectal cancers, older patients were less likely to have preoperative RT, and more likely to receive an AP resection compared to younger patients. The probability of undergoing preoperative RT and AP resection was reduced in females compared to males (odds ratio (OR) 0.77, 95% confidence interval (CI) 0.64-0.93 and OR 0.78, 95%CI 0.69-0.89, respectively). However, there was a trend of increasing RT over time (p for trend <0.01). The probability of undergoing AP resection was increased in less-educated patients and in hospitals with a low caseload.A higher risk of postoperative in-hospital mortality was found among colorectal cancer patients who were older, male, (female versus male OR 0.71, 95%CI 0.60-0.84), unmarried (OR 1.32, 95%CI 1.09-1.59) or with unknown marital status.
The study provides evidence of the importance of social, clinical and hospital characteristics on the equity and quality of care in a Southern European country with an open-access public health care system.
本研究旨在分析导致医疗管理和结果差异的社会、临床和医院特征。为此,使用行政数据调查了意大利西北部地区新诊断结直肠癌患者初始治疗质量的指标。
该队列包括通过验证算法从皮埃蒙特医院出院记录系统中选择的 8 年期间(2000-2007 年)所有新发结直肠癌患者(N=24187)。在这个基于人群的队列中评估了三个护理质量指标:直肠癌患者术前放疗(RT)和腹会阴切除术(AP)的比例,以及结直肠癌患者术后住院内死亡率的比例。
在直肠癌患者中,年龄较大的患者接受术前 RT 的可能性较小,而接受 AP 切除术的可能性较大。与男性相比,女性接受术前 RT 和 AP 切除术的可能性降低(比值比(OR)0.77,95%置信区间(CI)0.64-0.93 和 OR 0.78,95%CI 0.69-0.89)。然而,随着时间的推移,RT 的概率呈上升趋势(趋势检验 p<0.01)。受教育程度较低的患者和手术量较低的医院接受 AP 切除术的可能性增加。年龄较大、男性(女性与男性 OR 0.71,95%CI 0.60-0.84)、未婚(OR 1.32,95%CI 1.09-1.59)或婚姻状况不明的结直肠癌患者术后住院内死亡的风险较高。
该研究提供了证据,证明在一个具有开放获取公共医疗保健系统的南欧国家,社会、临床和医院特征对公平性和护理质量的重要性。