Jarboui Slim, Hlel Abdelwaheb, Daghfous Alifa, Bakkey Mohamed Ali, Sboui Imed
Department of General Surgery, Sidi Bouzid Hospital, 9132 Sidi Bouzid, Tunisia.
Case Rep Med. 2012;2012:484638. doi: 10.1155/2012/484638. Epub 2012 Aug 29.
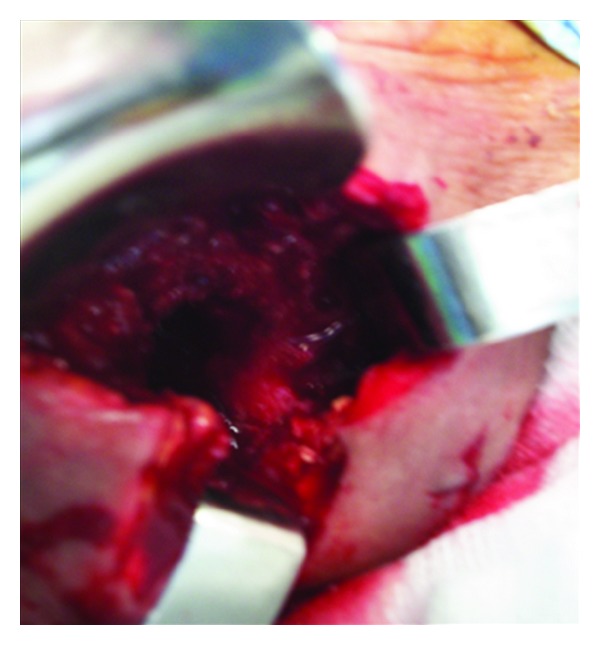
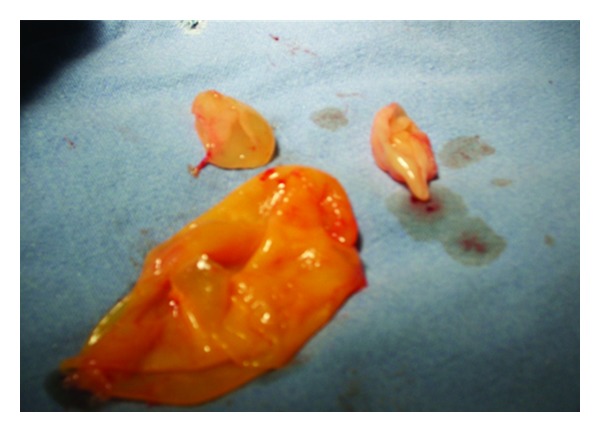
Cystic hydatid disease is a zoonosis caused by Echinococcus granulosus. It may affect any organ and tissue in the body, in particular the liver and Lung. Musculoskeletal or soft tissue hydatidosis accounts for about 0,5%-5% of all echinococcal infections in endemic areas and is almost secondary to the hepatic or pulmonary disease (Karaman et al., 2011; Dirican et al., 2008; Kouskos et al., 2007). Case Presentation. We report an unusual case of primary subcutaneous hydatidosis in the left supraclavicular region of the neck. A 53-year-old female patient was admitted with three-month history of pain and gradually growing mass located in the left supraclavicular region. Physical examination revealed a moderately hard, painful, and erythematous mass. The blood cell count was normal. Computed tomography demonstrated, a multilocular cystic lesion with thin borders and thin wall. The mass is binocular and extends to the scapula. CT showed no involvement of the lung. From these signs, the patient was diagnosed as having abscess (bacterial infection or tuberculosis). The diagnosis of Echinococcus granulosus infection was made per operatively after visualization of the cyst wall and the daughter cysts. Following irrigation of cystic cavity with hypertonic saline solution, the cyst wall was excised along with a portion of surrounding tissue. Histopathological examination of the specimen confirmed the hydatid origin. Hemagglutination tests for Echinococcus and ELISA were negative. Ultrasound of the abdomen was normal. The patient received albendazole (400 mg/day) for 8 weeks postoperatively. No sign of recurrence could be detected by physical examination and imaging (CT) at 4-month followup. Conclusion. The case illustrates that echinococcal disease should be considered in the differential diagnosis of every cystic mass in every anatomic location, especially when it occurs in endemic areas.
囊型包虫病是一种由细粒棘球绦虫引起的人畜共患病。它可累及身体的任何器官和组织,尤其是肝脏和肺。在流行地区,肌肉骨骼或软组织包虫病约占所有棘球绦虫感染的0.5%-5%,且几乎继发于肝脏或肺部疾病(卡拉曼等人,2011年;迪里坎等人,2008年;库斯科斯等人,2007年)。病例报告。我们报告一例罕见的原发性颈部左锁骨上区皮下包虫病病例。一名53岁女性患者因左锁骨上区疼痛伴肿块逐渐增大3个月入院。体格检查发现一个中度坚硬、疼痛且有红斑的肿块。血细胞计数正常。计算机断层扫描显示一个边界薄且壁薄的多房囊性病变。肿块呈双眼状并延伸至肩胛骨。CT显示肺部未受累。根据这些体征,患者被诊断为脓肿(细菌感染或结核病)。在术中观察到囊肿壁和子囊后,确诊为细粒棘球绦虫感染。用高渗盐溶液冲洗囊腔后,切除囊肿壁及周围部分组织。标本的组织病理学检查证实为包虫起源。棘球绦虫血凝试验和酶联免疫吸附测定均为阴性。腹部超声检查正常。患者术后接受阿苯达唑(400毫克/天)治疗8周。在4个月的随访中,体格检查和影像学检查(CT)均未发现复发迹象。结论。该病例表明,在对每个解剖部位的每个囊性肿块进行鉴别诊断时,尤其是在流行地区出现时,应考虑棘球绦虫病。