Department of Respiratory Medicine, Atrium Medical Centre, Heerlen, The Netherlands.
BMC Pulm Med. 2012 Sep 14;12:57. doi: 10.1186/1471-2466-12-57.
(18)F-FDG PET/CT (PET) is useful in assessing inflammatory activity in sarcoidosis. However, no appropriate indications are available. The aim of this study was to develop a prediction rule that can be used to identify symptomatic sarcoidosis patients who have a high probability of PET-positivity.
We retrospectively analyzed a cohort of sarcoidosis patients with non organ specific persistent disabling symptoms (n = 95). Results of soluble interleukin-2 receptor (sIL-2R) assessment and high-resolution computed tomography (HRCT) were included in the predefined model. HRCT scans were classified using a semi-quantitative scoring system and PET findings as positive or negative, respectively. A prediction model was derived based on logistic regression analysis. We quantified the model's performance using measures of discrimination and calibration. Finally, we constructed a prediction rule that should be easily applicable in clinical practice.
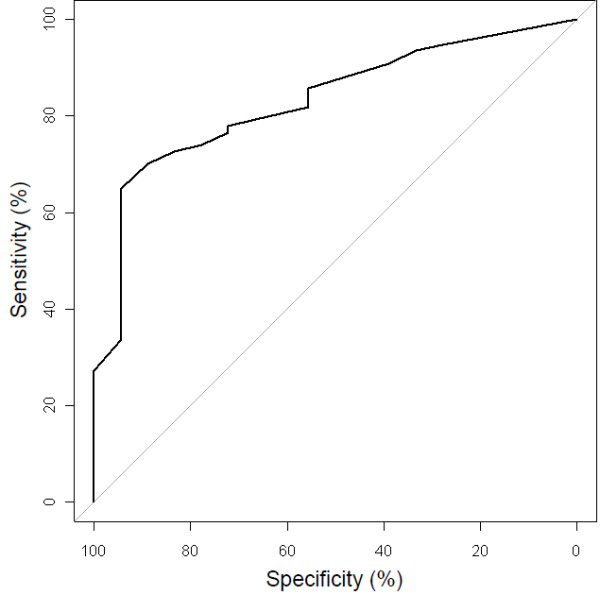
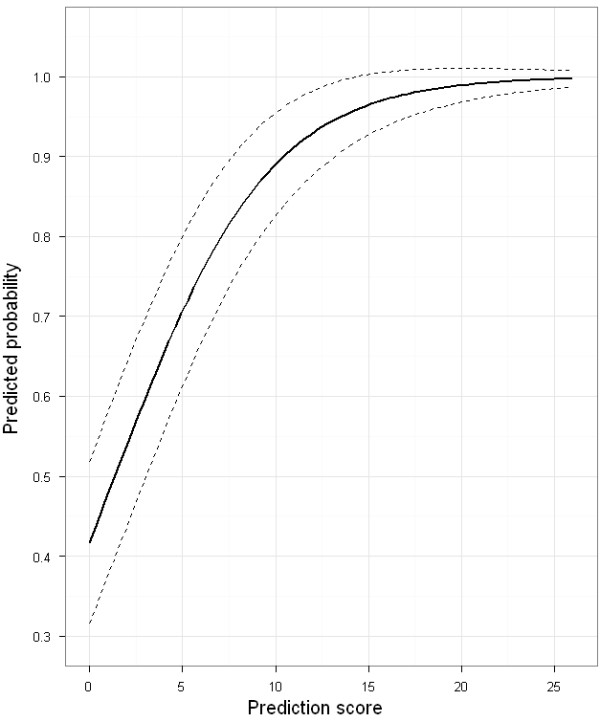
The prediction rule showed good calibration and good overall performance (goodness-of-fit test, p = 0.78, Brier score 20.1%) and discriminated between patients with positive and negative PET findings (area under the receiver-operating characteristic curve, 0.83). If a positive predictive value for the presence of inflammatory activity of ≥90% is considered acceptable for clinical decision-making without referral to PET, PET would be indicated in only 29.5% of the patients. Using a positive predictive value of 98%, about half of the patients (46.3%) would require referral to PET.
The derived and internally validated clinical prediction rule, based on sIL-2R levels and HRCT scoring results, appeared to be useful to identify sarcoidosis patients with a high probability of inflammatory activity. Using this rule may enable a more effective use of PET scan for assessment of inflammatory activity in sarcoidosis.
(18)F-FDG PET/CT(PET)在评估结节病的炎症活性方面很有用。但是,目前尚无明确的适应证。本研究旨在制定一个预测规则,以识别具有高 PET 阳性可能性的有症状结节病患者。
我们回顾性分析了一组患有非器官特异性持续性致残症状的结节病患者队列(n=95)。可溶性白细胞介素-2 受体(sIL-2R)评估和高分辨率计算机断层扫描(HRCT)的结果包含在预设模型中。HRCT 扫描使用半定量评分系统进行分类,分别将 PET 结果定义为阳性或阴性。基于逻辑回归分析得出预测模型。我们使用区分度和校准度指标来量化模型的性能。最后,我们构建了一个易于在临床实践中应用的预测规则。
该预测规则显示出良好的校准度和整体性能(拟合优度检验,p=0.78,Brier 评分 20.1%),并能区分 PET 结果阳性和阴性的患者(接受者操作特征曲线下面积,0.83)。如果将≥90%的炎症活性阳性预测值作为无 PET 检查的临床决策的可接受标准,那么只有 29.5%的患者需要进行 PET 检查。如果使用阳性预测值为 98%,则约一半(46.3%)的患者需要转诊至 PET 检查。
基于 sIL-2R 水平和 HRCT 评分结果得出的内部验证预测规则,似乎可用于识别炎症活性可能性较高的结节病患者。使用该规则可能使 PET 扫描在评估结节病的炎症活性方面的应用更加有效。