Department of Environmental Health, Rollins School of Public Health, Emory University, 1518 Clifton Road NE, Atlanta, GA 30322, USA.
Environ Health. 2012 Sep 21;11:70. doi: 10.1186/1476-069X-11-70.
Emergency department (ED) visit and hospital admissions (HA) data have been an indispensible resource for assessing acute morbidity impacts of air pollution. ED visits and HAs are types of health care visits with similarities, but also potentially important differences. Little previous information is available regarding the impact of health care visit type on observed acute air pollution-health associations from studies conducted for the same location, time period, outcome definitions and model specifications.
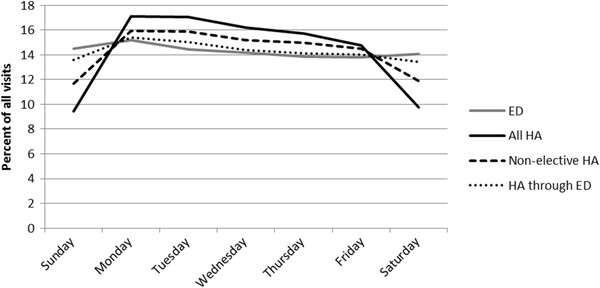
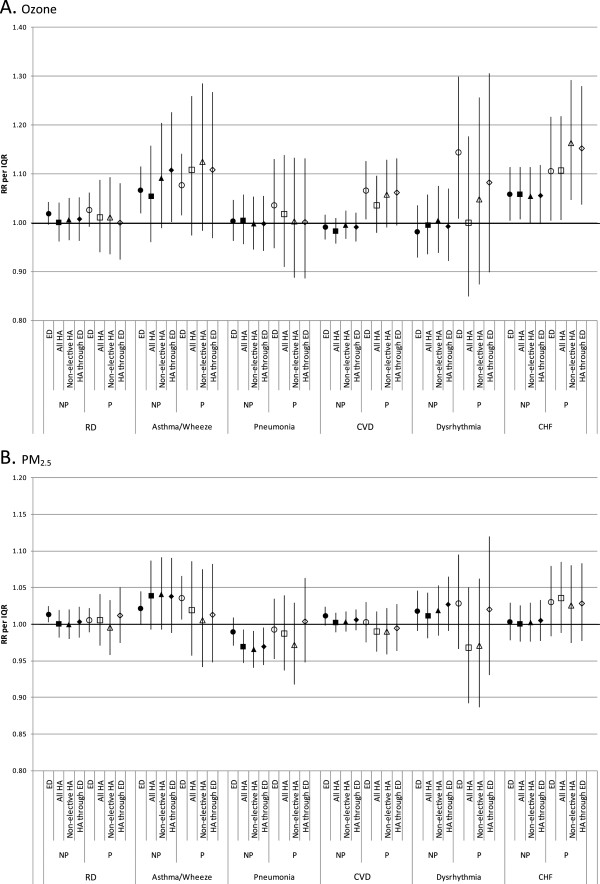
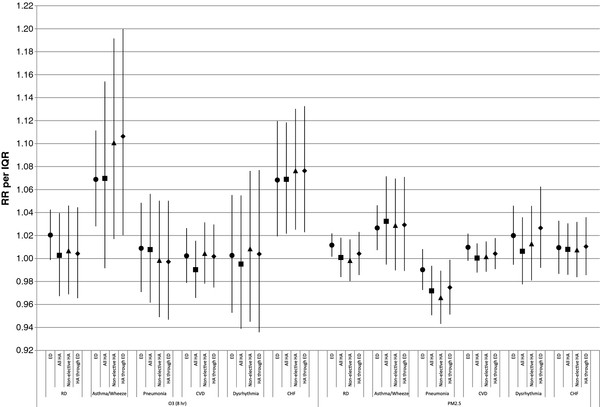
As part of a broader study of air pollution and health in St. Louis, individual-level ED and HA data were obtained for a 6.5 year period for acute care hospitals in the eight Missouri counties of the St. Louis metropolitan area. Patient demographic characteristics and diagnostic code distributions were compared for four visit types including ED visits, HAs, HAs that came through the ED, and non-elective HAs. Time-series analyses of the relationship between daily ambient ozone and PM₂.₅ and selected cardiorespiratory outcomes were conducted for each visit type.
Our results indicate that, compared with ED patients, HA patients tended to be older, had evidence of greater severity for some outcomes, and had a different mix of specific outcomes. Consideration of 'HA through ED' appeared to more effectively select acute visits than consideration of 'non-elective HA'. While outcomes with the strongest observed temporal associations with air pollutants tended to show strong associations for all visit types, we found some differences in observed associations for ED visits and HAs. For example, risk ratios for the respiratory disease-ozone association were 1.020 for ED visits and 1.004 for 'HA through ED'; risk ratios for the asthma/wheeze-ozone association were 1.069 for ED visits and 1.106 for 'HA through ED'. Several factors (e.g. age) were identified that may be responsible, in part, for the differences in observed associations.
Demographic and diagnostic differences between visit types may lead to preference for one visit type over another for some questions and populations. The strengths of observed associations with air pollutants sometimes varied between different health care visit types, but the relative strengths of association generally were specific to the pollutant-outcome combination.
急诊科(ED)就诊和住院(HA)数据是评估空气污染急性发病影响的不可或缺的资源。ED 就诊和 HA 是具有相似性的医疗保健就诊类型,但也可能存在重要差异。之前几乎没有关于就诊类型对同一地点、同一时间段、相同结果定义和模型规范的研究中观察到的急性空气污染-健康关联的影响的信息。
作为圣路易斯地区空气污染和健康研究的一部分,在密苏里州圣路易斯大都市区的 8 个县的急性护理医院获得了为期 6.5 年的个体层面的 ED 和 HA 数据。比较了四种就诊类型(ED 就诊、HA、通过 ED 的 HA 和非择期 HA)的患者人口统计学特征和诊断代码分布。对每种就诊类型的每日环境臭氧和 PM₂.₅与选定的心肺疾病结局之间的关系进行了时间序列分析。
我们的结果表明,与 ED 患者相比,HA 患者往往年龄更大,一些结局的严重程度更高,且特定结局的组合也不同。考虑“通过 ED 的 HA”比考虑“非择期 HA”更能有效地选择急性就诊。虽然与空气污染物具有最强观察到的时间关联的结局往往对所有就诊类型都显示出很强的关联,但我们发现 ED 就诊和 HA 之间的观察到的关联存在一些差异。例如,呼吸道疾病-臭氧关联的风险比为 ED 就诊的 1.020 和“通过 ED 的 HA”的 1.004;哮喘/喘息-臭氧关联的风险比为 ED 就诊的 1.069 和“通过 ED 的 HA”的 1.106。确定了一些因素(例如年龄)可能部分解释了观察到的关联差异。
就诊类型之间的人口统计学和诊断差异可能导致某些问题和人群对某一种就诊类型的偏好。与空气污染物的观察到的关联强度有时在不同的医疗保健就诊类型之间有所不同,但关联的相对强度通常特定于污染物-结局组合。