Department of Community Health Sciences, University of Calgary, Calgary, Alberta, Canada.
Int J Health Geogr. 2012 Oct 3;11:42. doi: 10.1186/1476-072X-11-42.
Evaluating geographic access to health services often requires determining the patient travel time to a specified service. For urgent care, many research studies have modeled patient pre-hospital time by ground emergency medical services (EMS) using geographic information systems (GIS). The purpose of this study was to determine if the modeling assumptions proposed through prior United States (US) studies are valid in a non-US context, and to use the resulting information to provide revised recommendations for modeling travel time using GIS in the absence of actual EMS trip data.
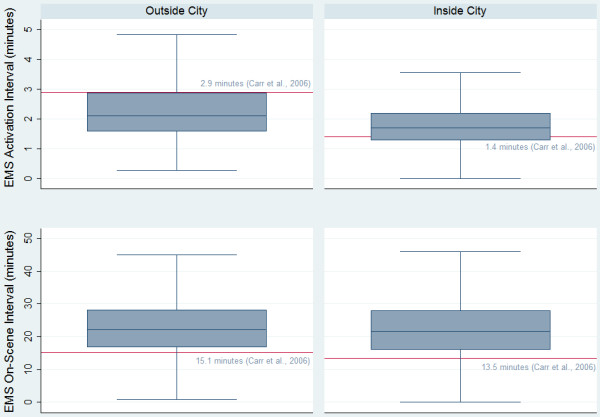
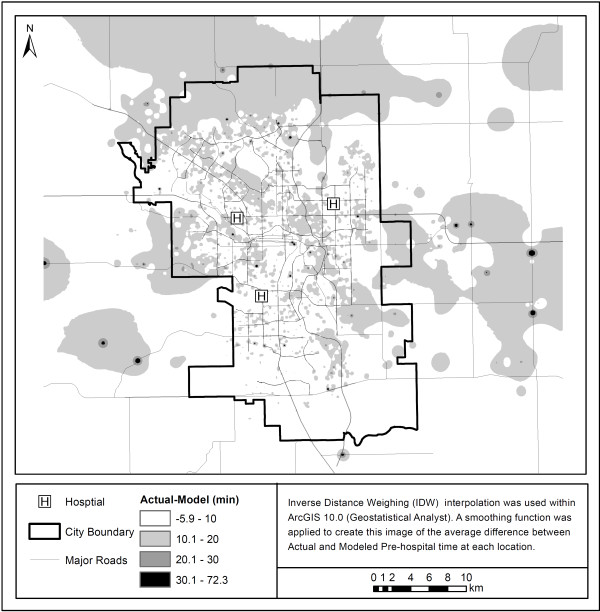
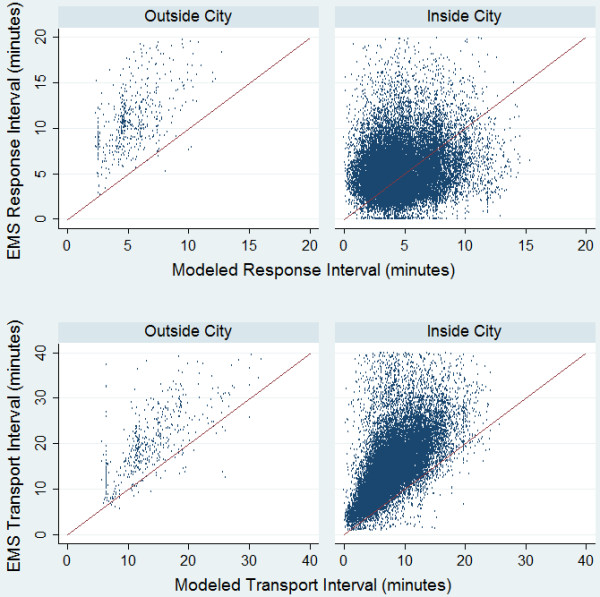
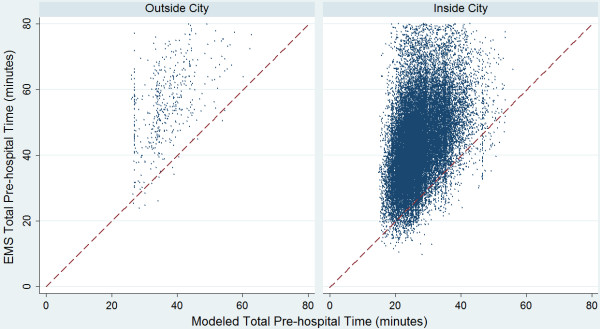
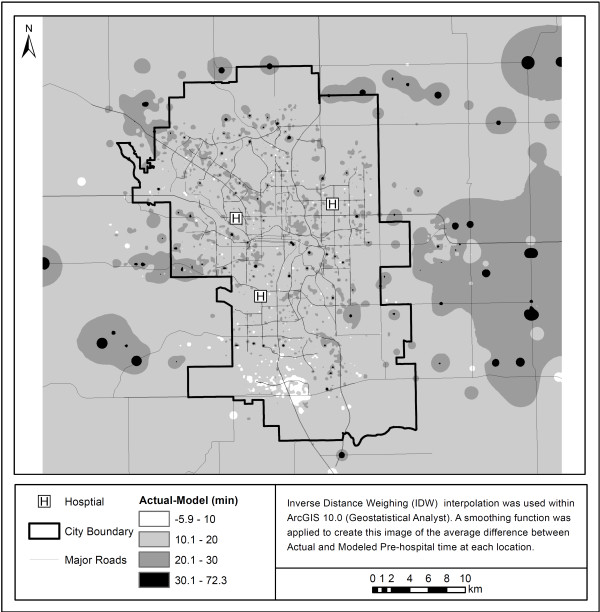
The study sample contained all emergency adult patient trips within the Calgary area for 2006. Each record included four components of pre-hospital time (activation, response, on-scene and transport interval). The actual activation and on-scene intervals were compared with those used in published models. The transport interval was calculated within GIS using the Network Analyst extension of Esri ArcGIS 10.0 and the response interval was derived using previously established methods. These GIS derived transport and response intervals were compared with the actual times using descriptive methods. We used the information acquired through the analysis of the EMS trip data to create an updated model that could be used to estimate travel time in the absence of actual EMS trip records.
There were 29,765 complete EMS records for scene locations inside the city and 529 outside. The actual median on-scene intervals were longer than the average previously reported by 7-8 minutes. Actual EMS pre-hospital times across our study area were significantly higher than the estimated times modeled using GIS and the original travel time assumptions. Our updated model, although still underestimating the total pre-hospital time, more accurately represents the true pre-hospital time in our study area.
The widespread use of generalized EMS pre-hospital time assumptions based on US data may not be appropriate in a non-US context. The preference for researchers should be to use actual EMS trip records from the proposed research study area. In the absence of EMS trip data researchers should determine which modeling assumptions more accurately reflect the EMS protocols across their study area.
评估医疗服务的地理可达性通常需要确定患者到达指定服务的出行时间。对于紧急护理,许多研究使用地理信息系统 (GIS) 通过地面紧急医疗服务 (EMS) 对患者的院前时间进行建模。本研究的目的是确定美国 (US) 之前的研究提出的建模假设在非 US 环境中是否有效,并利用这些信息为在缺乏实际 EMS 行程数据的情况下使用 GIS 建模出行时间提供修订建议。
研究样本包含 2006 年卡尔加里地区所有的急诊成年患者出行记录。每条记录包括院前时间的四个组成部分(激活、响应、现场和运输间隔)。实际的激活和现场间隔与已发表模型中的间隔进行了比较。在 GIS 中使用 Esri ArcGIS 10.0 的 Network Analyst 扩展计算了运输间隔,使用先前建立的方法得出了响应间隔。使用描述性方法比较了这些 GIS 派生的运输和响应间隔与实际时间。我们利用通过分析 EMS 行程数据获得的信息创建了一个更新的模型,可以在缺乏实际 EMS 行程记录的情况下用于估计出行时间。
在城市内部和外部的场景位置,共有 29765 个完整的 EMS 记录。实际的中位数现场间隔比之前报告的平均时间长 7-8 分钟。我们研究区域内的实际 EMS 院前时间明显高于使用 GIS 和原始出行时间假设建模的估计时间。我们的更新模型虽然仍然低估了总院前时间,但更准确地代表了我们研究区域内的真实院前时间。
基于美国数据的广泛使用通用 EMS 院前时间假设在非 US 环境中可能并不合适。研究人员的首选应该是使用拟议研究区域的实际 EMS 行程记录。在缺乏 EMS 行程数据的情况下,研究人员应确定哪些建模假设更能反映整个研究区域的 EMS 协议。