Department of Emergency Medicine & Internal Medicine, Hennepin County Medical Center, Minneapolis, Minnesota, USA.
BMJ Open. 2012 Oct 3;2(5). doi: 10.1136/bmjopen-2012-001273. Print 2012.
To determine whether the use of cardiocerebral resuscitation (CCR) or AHA/ERC 2005 Resuscitation Guidelines improved patient outcomes from out-of-hospital cardiac arrest (OHCA) compared to older guidelines.
Systematic review and meta-analysis.
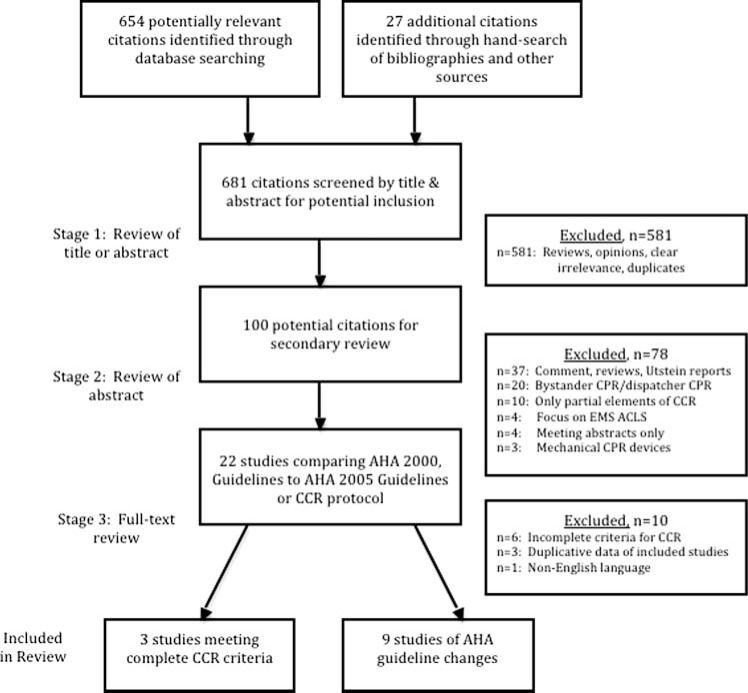
MEDLINE, EMBASE, Web of Science and the Cochrane Library databases. We also hand-searched study references and consulted experts.
Design: randomised controlled trials and observational studies.
OHCA patients, age >17 years.
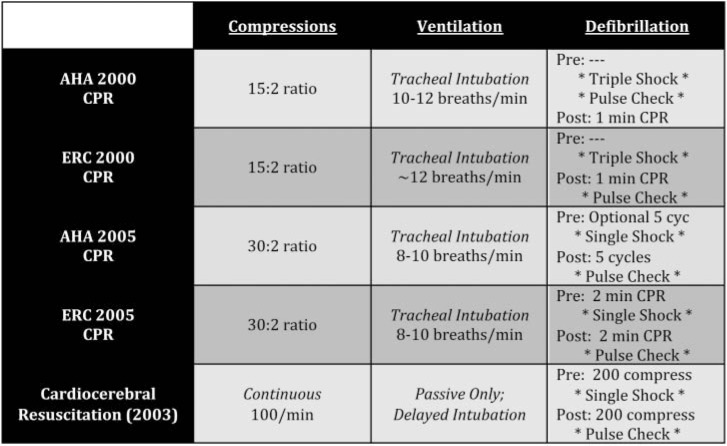
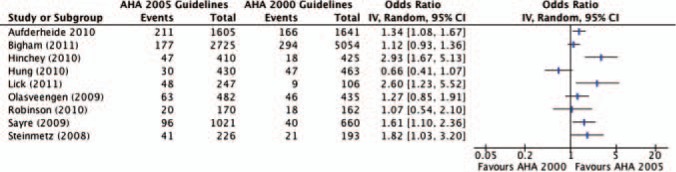
'Control' protocol versus 'Study' protocol. 'Control' protocol defined as AHA/ERC 2000 Guidelines for cardiopulmonary resuscitation (CPR). 'Study' protocol defined as AHA/ERC 2005 Guidelines for CPR, or a CCR protocol.
Survival to hospital discharge.
High-quality or medium-quality studies, as measured by the Newcastle Ottawa Scale using predefined categories.
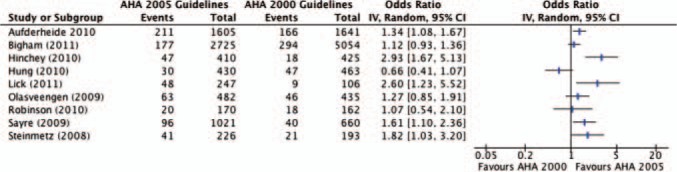
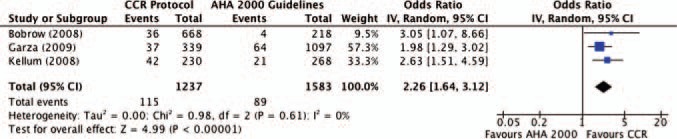
Twelve observational studies met inclusion criteria. All the three studies using CCR demonstrated significantly improved survival compared to use of AHA 2000 Guidelines, as did five of the nine studies using AHA/ERC 2005 Guidelines. Pooled data demonstrate that use of a CCR protocol has an unadjusted OR of 2.26 (95% CI 1.64 to 3.12) for survival to hospital discharge among all cardiac arrest patients. Among witnessed ventricular fibrillation/ventricular tachycardia (VF/VT) patients, CCR increased survival by an OR of 2.98 (95% CI 1.92 to 4.62). Studies using AHA/ERC 2005 Guidelines showed an overall trend towards increased survival, but significant heterogeneity existed among these studies.
We demonstrate an association with improved survival from OHCA when CCR protocols or AHA/ERC 2005 Guidelines are compared to use of older guidelines. In the subgroup of patients with witnessed VF/VT, there was a threefold increase in OHCA survival when CCR was used. CCR appears to be a promising resuscitation protocol for Emergency Medical Services providers in increasing survival from OHCA. Future research will need to be conducted to directly compare AHA/ERC 2010 Guidelines with the CCR approach.
比较心肺复苏(CCR)或 AHA/ERC 2005 复苏指南与旧指南,以确定使用前者是否能改善院外心脏骤停(OHCA)患者的预后。
系统评价和荟萃分析。
MEDLINE、EMBASE、Web of Science 和 Cochrane 图书馆数据库。我们还进行了手工检索研究参考文献并咨询了专家。
设计:随机对照试验和观察性研究。
OHCA 患者,年龄>17 岁。
“对照组”方案与“研究组”方案。“对照组”方案定义为 AHA/ERC 2000 心肺复苏(CPR)指南。“研究组”方案定义为 AHA/ERC 2005 CPR 指南或 CCR 方案。
存活至出院。
采用纽卡斯尔-渥太华量表(Newcastle Ottawa Scale),根据预先设定的类别,对高质量或中质量研究进行评估。
符合纳入标准的有 12 项观察性研究。与使用 AHA 2000 指南相比,所有使用 CCR 的三项研究均显著提高了生存率,使用 AHA/ERC 2005 指南的九项研究中有五项也显示出了同样的结果。汇总数据表明,在所有心脏骤停患者中,使用 CCR 方案的调整后比值比(OR)为 2.26(95%置信区间 1.64 至 3.12),用于存活至出院。在目击的心室颤动/心室心动过速(VF/VT)患者中,CCR 将生存率提高了 2.98(95%置信区间 1.92 至 4.62)。使用 AHA/ERC 2005 指南的研究显示出了生存率提高的总体趋势,但这些研究之间存在显著的异质性。
与使用旧指南相比,当 CCR 方案或 AHA/ERC 2005 指南与使用旧指南相比时,我们证明了 OHCA 患者的生存率存在关联。在目击的 VF/VT 患者亚组中,使用 CCR 可使 OHCA 生存率提高三倍。CCR 似乎是一种有前途的复苏方案,可为急诊医疗服务提供者增加 OHCA 患者的生存率。未来的研究需要直接比较 AHA/ERC 2010 指南与 CCR 方法。